
Cardiovascular — MCQs

On this page
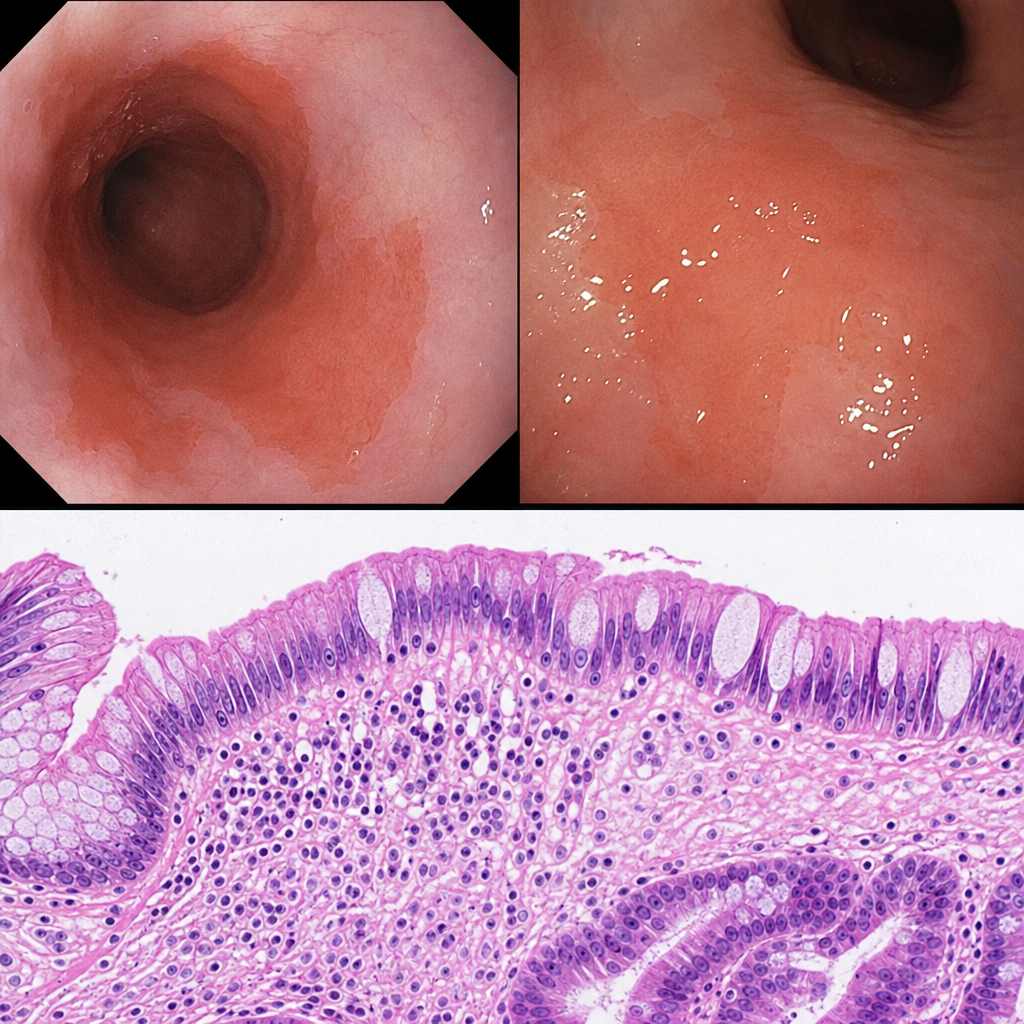
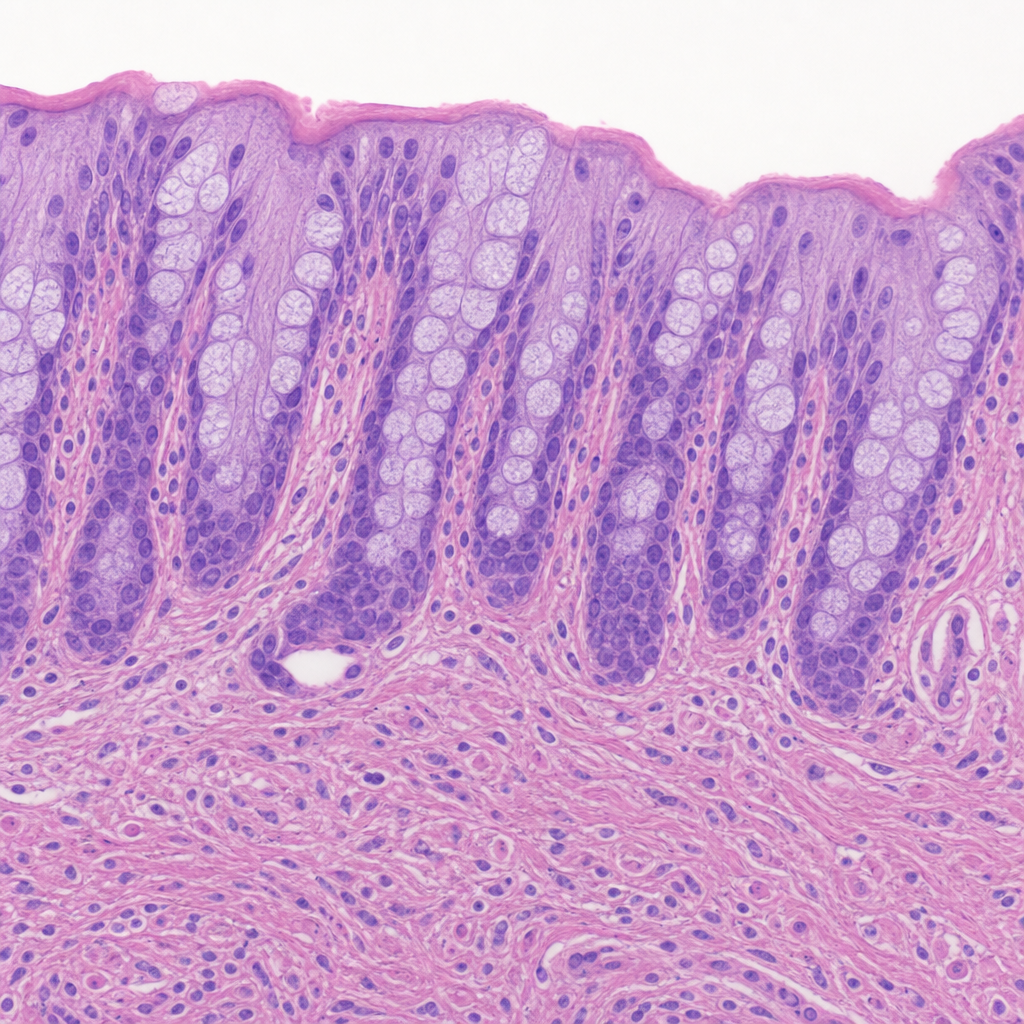
A 67-year-old man with a long-standing history of gastroesophageal reflux disease undergoes upper endoscopy. A biopsy from 2 cm above the gastroesophageal junction is obtained from an area of salmon-colored mucosa. Histological examination shows replacement of the normal squamous epithelium by columnar epithelium containing goblet cells interspersed among columnar absorptive cells, with intact basement membrane and no nuclear stratification, pleomorphism, or loss of polarity. Which of the following statements most accurately characterizes the biological behavior and reversibility of this histological change?
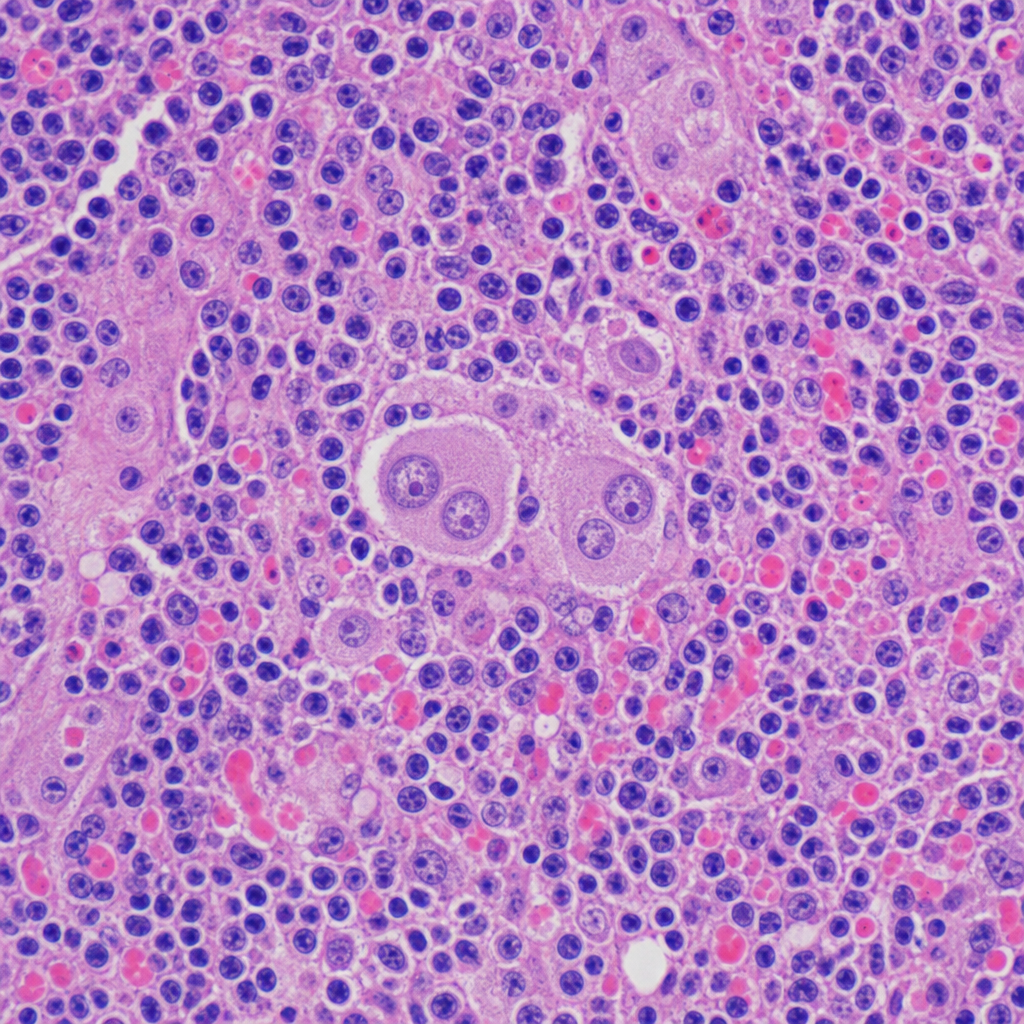
A 34-year-old woman presents with fatigue, night sweats, and painless cervical lymphadenopathy. Excisional biopsy of a cervical lymph node is performed. Large binucleate cells with prominent eosinophilic 'owl-eye' nucleoli are surrounded by a mixed inflammatory background of lymphocytes, eosinophils, plasma cells, and neutrophils. Which of the following cell types is the neoplastic cell of origin responsible for generating the observed inflammatory microenvironment?
A 58-year-old man with a long history of gastroesophageal reflux disease undergoes upper endoscopy. A biopsy is taken from the distal esophagus. The photomicrograph shows replacement of the normal stratified squamous epithelium by columnar epithelium with goblet cells. The patient is counseled that this change carries an increased risk of malignant transformation. Which of the following best describes the reversibility of the currently observed change and the next step in the malignant progression sequence?
A 14-year-old Caucasian female with a family history of familial hypercholesterolemia commits suicide by drug overdose. Her family decides to donate her organs, and her heart is removed for donation. After removing the heart, the cardiothoracic surgeon notices flat yellow spots on the inside of her aorta. Which of the following cell types predominate in these yellow spots?
A 51-year-old man comes to the physician for the evaluation of a 3-week history of fatigue and shortness of breath. One year ago, a screening colonoscopy showed colonic polyps. His brother has a bicuspid aortic valve. On examination, a late systolic crescendo-decrescendo murmur is heard at the right upper sternal border. Laboratory studies show: Hemoglobin 9.1 g/dL LDH 220 U/L Haptoglobin 25 mg/dL (N = 41–165 mg/dL) Urea nitrogen 22 mg/dL Creatinine 1.1 mg/dL Total bilirubin 1.8 mg/dL A peripheral blood smear shows schistocytes. Which of the following is the most likely cause of this patient's anemia?
Practice by Chapter
Atherosclerosis
Practice Questions
Ischemic heart disease
Practice Questions
Myocardial infarction pathology
Practice Questions
Hypertensive heart disease
Practice Questions
Congenital heart defects
Practice Questions
Valvular heart disease
Practice Questions
Rheumatic heart disease
Practice Questions
Infective endocarditis
Practice Questions
Myocarditis and cardiomyopathies
Practice Questions
Pericardial diseases
Practice Questions
Aneurysms and dissections
Practice Questions
Vasculitis
Practice Questions
Cardiac tumors
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app