
Third stage of labor — MCQs

A clinical diagnosis of abruptio placentae is suspected. Which of the following is the most appropriate next step in the management of this patient?
Immediately following prolonged delivery of the placenta at 40 weeks gestation, a 32-year-old multiparous woman develops vaginal bleeding. Other than mild asthma, the patient’s pregnancy has been uncomplicated. She has attended many prenatal appointments and followed the physician's advice about screening for diseases, laboratory testing, diet, and exercise. Previous pregnancies were uncomplicated. She has no history of a serious illness. She is currently on intravenous infusion of oxytocin. Her temperature is 37.2°C (99.0°F), blood pressure is 108/60 mm Hg, pulse is 88/min, and respirations are 17/min. Uterine palpation reveals a soft enlarged fundus that extends above the umbilicus. Based on the assessment of the birth canal and placenta, which of the following options is the most appropriate initial step in patient management?
A 34-year-old G5P5 woman gave birth to a healthy infant 30 minutes ago by vacuum-assisted vaginal delivery and is now experiencing vaginal bleeding. The placenta was delivered spontaneously and was intact upon examination. The infant weighed 5.2 kg and had Apgar scores of 8 and 9. No perineal tear or intentional episiotomy occurred. The patient has type 1 diabetes. She had good glycemic control throughout her pregnancy. She took a prenatal vitamin daily. Blood pressure is 135/72 mmHg, pulse is 102/min, and respirations are 18/min. Upon physical examination, the uterine fundus is soft and palpated 4 cm above the umbilicus. There are 3-cm blood clots on the patient’s bed pad. Which of the following is the next best step in management for the patient’s bleeding?
A 29-year-old G1P0 female at 32 weeks gestation presents to the emergency department with vaginal bleeding. She has had minimal prenatal care to-date with only an initial visit with an obstetrician after a positive home pregnancy test. She describes minimal spotting that she noticed earlier today that has progressed to larger amounts of blood; she estimates 30 mL of blood loss. She denies any cramping, pain, or contractions, and she reports feeling continued movements of the baby. Ultrasound and fetal heart rate monitoring confirm the presence of a healthy fetus without any evidence of current or impending complications. The consulted obstetrician orders blood testing for Rh-status of both the mother as well as the father, who brought the patient to the hospital. Which of the following represents the best management strategy for this situation?
A 37-year-old woman, gravida 4, para 3, at 35 weeks' gestation is admitted to the hospital in active labor. Her three children were delivered by Cesarean section. One hour after vaginal delivery, the placenta is not delivered. Manual separation of the placenta leads to profuse vaginal bleeding. Her pulse is 122/min and blood pressure is 90/67 mm Hg. A firm, nontender uterine fundus is palpated at the level of the umbilicus. Hemoglobin is 8.3 g/dL and platelet count is 220,000/mm3. Activated partial thromboplastin time and prothrombin time are within normal limits. Which of the following is the most likely underlying mechanism of this patient's postpartum bleeding?
A 25-year-old G2P1001 at 32 weeks gestation presents to the hospital with painless vaginal bleeding. The patient states that she was taking care of laundry at home when she experienced a sudden sensation of her water breaking and saw that her groin was covered in blood. Her prenatal history is unremarkable according to the clinic records, but she has not seen an obstetrician for the past 14 weeks. Her previous delivery was by urgent cesarean section for placenta previa. Her temperature is 95°F (35°C), blood pressure is 125/75 mmHg, pulse is 79/min, respirations are 18/min, and oxygen saturation is 98% on room air. Cervical exam shows gross blood in the vaginal os. The fetal head is not palpable. Fetal heart rate monitoring demonstrates decelerations and bradycardia. Labs are pending. IV fluids are started. What is the best next step in management?
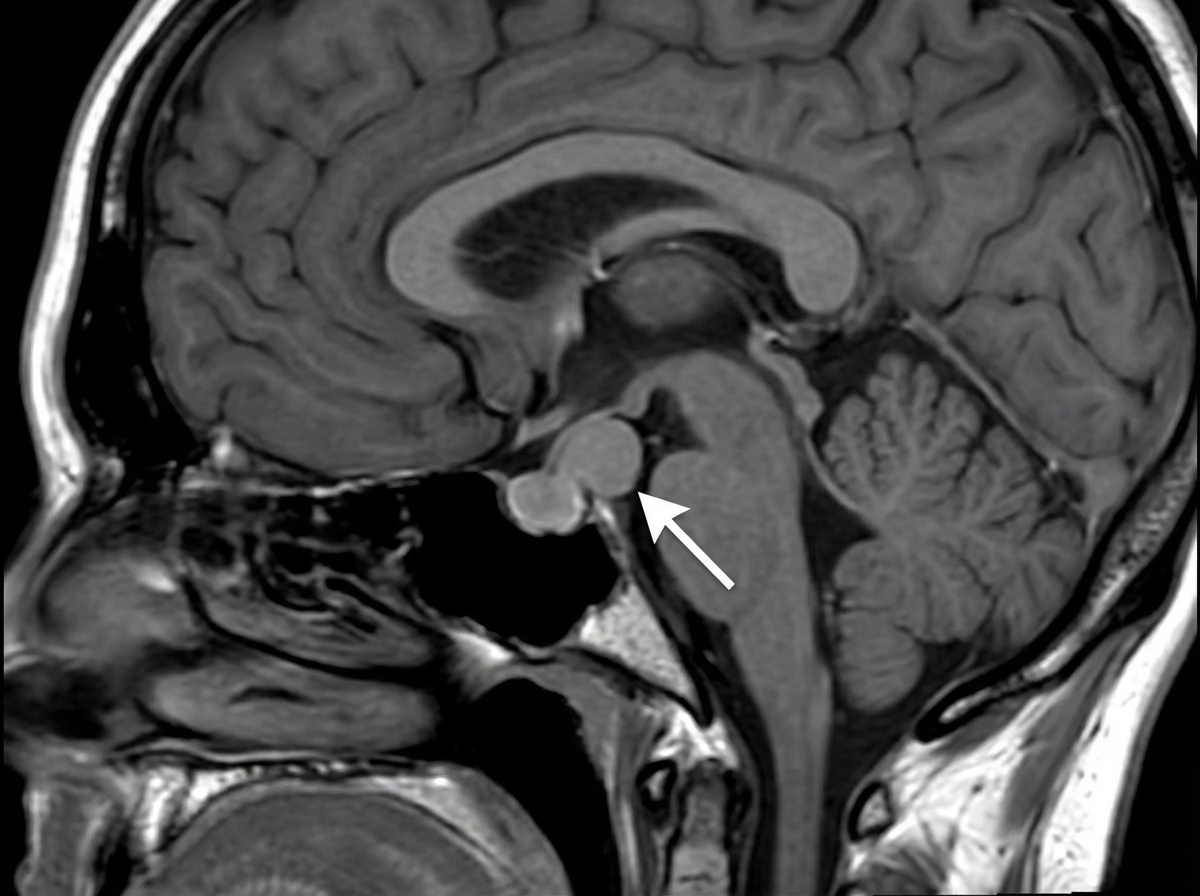
A 17-year-old teenager presents to the clinic with her parents complaining of headaches and loss of vision which began insidiously 3 months ago. She describes her headaches as throbbing, mostly on her forehead, and severe enough to affect her daily activities. She has not experienced menarche. Past medical history is noncontributory. She takes no medication. Both of her parents are alive and well. Today, her blood pressure is 110/70 mm Hg, the heart rate is 90/min, the respiratory rate is 17/min, and the temperature is 37.0°C (98.6°F). Breasts and pubic hair development are in Tanner stage I. Blood work is collected and an MRI is performed (the result is shown). Decreased production of which of the following hormones is the most likely explanation for the patient's signs and symptoms?
A 54-year-old male comes to the clinic to initiate care with a new physician. He has no complaints at this time. When taking his history, the patient says his medical history is notable for diabetes and hypertension both of which are well managed on his medications. His medications are metformin and lisinopril. A review of systems is negative. While taking the social history, the patient hesitates when asked about alcohol consumption. Further gentle questioning by the physician leads the patient to admit that he drinks 5-6 beers per night and up to 10-12 drinks per day over the weekend. He says that he has been drinking like this for “years.” He becomes emotional and says that his alcohol is negatively affecting his relationship with his wife and children; however, when asked about efforts to decrease his consumption, the patient says he has not tried in the past and doesn’t think he has “the strength to stop”. Which of the following stages of change most accurately describes this patient’s behavior?
A 30-year-old woman, gravida 2, para 1, at 38 weeks' gestation comes to the hospital for regular, painful contractions that have been increasing in frequency. Her pregnancy has been complicated by gestational diabetes treated with insulin. Pelvic examination shows the cervix is 50% effaced and 4 cm dilated; the vertex is at -1 station. Ultrasonography shows no abnormalities. A tocometer and Doppler fetal heart monitor are placed on the patient's abdomen. The fetal heart rate monitoring strip shows a baseline heart rate of 145/min with a variability of ≥ 15/min. Within a 20-minute recording, there are 7 uterine contractions, 4 accelerations, and 3 decelerations that have a nadir occurring within half a minute. The decelerations occur at differing intervals relative to the contractions. Which of the following is the most appropriate next step in the management of this patient?
A 25-year-old G1P0000 presents to her obstetrician’s office for a routine prenatal visit at 32 weeks gestation. At this visit, she feels well and has no complaints. Her pregnancy has been uncomplicated, aside from her Rh negative status, for which she received Rhogam at 28 weeks gestation. The patient has a past medical history of mild intermittent asthma and migraine headaches. She currently uses her albuterol inhaler once a week and takes a prenatal vitamin. Her temperature is 98.6°F (37.0°C), pulse is 70/min, blood pressure is 117/68 mmHg, and respirations are 13/min. Cardiopulmonary exam is unremarkable, and abdominal exam reveals a gravid uterus with fundal height at 30 centimeters. Bedside ultrasound reveals that the fetus is in transverse lie. The patient states that she prefers to have a vaginal delivery. Which of the following is the best next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app