
Labor curve and Friedman curve — MCQs

You have been entrusted with the task of finding the causes of low birth weight in infants born in the health jurisdiction for which you are responsible. In 2017, there were 1,500 live births and, upon further inspection of the birth certificates, 108 of these children had a low birth weight (i.e. lower than 2,500 g), while 237 had mothers who smoked continuously during pregnancy. Further calculations have shown that the risk of low birth weight in smokers was 14% and in non-smokers, it was 7%, while the relative risk of low birth weight linked to cigarette smoking during pregnancy was 2%. In other words, women who smoked during pregnancy were twice as likely as those who did not smoke to deliver a low-weight infant. Using this data, you are also asked to calculate how much of the excess risk for low birth weight, in percentage terms, can be attributed to smoking. What is the attributable risk percentage for smoking leading to low birth weight?
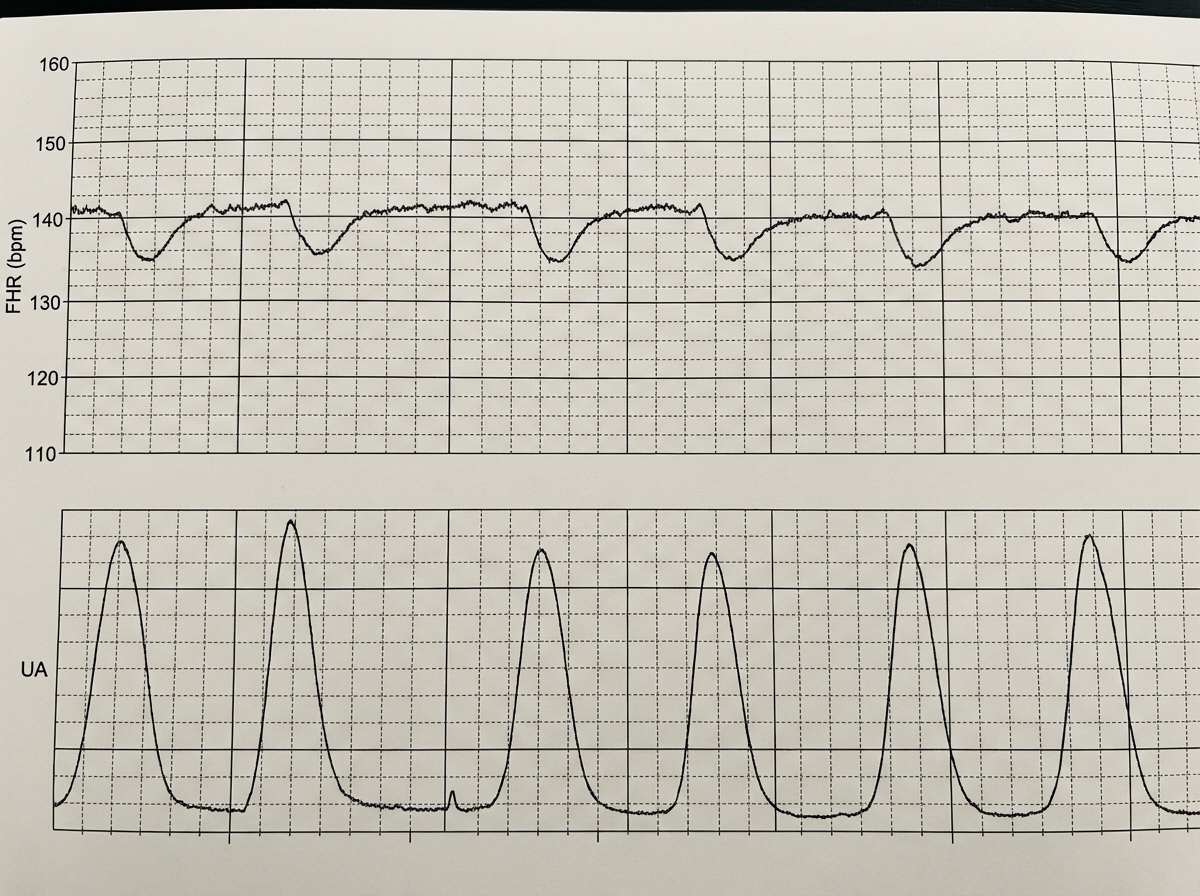
A 39-year-old woman, gravida 5, para 4, at 41 weeks' gestation is brought to the hospital because of regular uterine contractions that started 2 hours ago. Pregnancy has been complicated by iron deficiency anemia treated with iron supplements. Pelvic examination shows the cervix is 90% effaced and 7-cm dilated; the vertex is at -1 station. Fetal heart tracing is shown. The patient is repositioned, O2 therapy is initiated, and amnioinfusion is done. A repeat assessment after 20 minutes shows a similar cervical status, and no changes in the fetal heart tracing, and less than 5 contractions in a period of 10 minutes.What is the most appropriate next step in management?
A 30-year-old G3P0 woman who is 28 weeks pregnant presents for a prenatal care visit. She reports occasionally feeling her baby move but has not kept count over the past couple weeks. She denies any bleeding, loss of fluid, or contractions. Her previous pregnancies resulted in spontaneous abortions at 12 and 14 weeks. She works as a business executive, has been in excellent health, and has had no surgeries. She states that she hired a nutritionist and pregnancy coach to ensure good prospects for this pregnancy. On physical exam, fetal heart tones are not detected. Abdominal ultrasound shows a 24-week fetal demise. The patient requests an autopsy on the fetus and wishes for the fetus to pass "as naturally as possible." What is the best next step in management?
A 38-year-old woman, gravida 4, para 3, at 20 weeks' gestation comes to the physician for a prenatal care visit. She used fertility enhancing treatment for her current pregnancy. Her other children were born before 37 weeks' gestation. She is 170 cm (5 ft 7 in) tall and weighs 82 kg (180 lb); BMI is 28.4 kg/m2. Her vital signs are within normal limits. The abdomen is nontender, and no contractions are felt. Ultrasonography shows a cervical length of 22 mm and a fetal heart rate of 140/min. Which of the following is the most likely diagnosis?
A 30-year-old woman, gravida 2 para 1, at 39 weeks gestation presents to the hospital with painful contractions and a rupture of membranes. She reports that the contractions started a couple hours ago and are now occurring every 4 minutes. She is accompanied by her husband who states, “her water broke an hour ago before we left for the hospital." The patient denies vaginal bleeding, and fetal movements are normal. The patient has attended all her pre-natal visits without pregnancy complications. She has no chronic medical conditions and takes only pre-natal vitamins. Her blood pressure is 110/75 mm Hg and pulse is 82/min. A fetal heart rate tracing shows a pulse of 140/min with moderate variability and no decelerations. Cervical examination reveals a cervix that is 7 cm dilated and 100% effaced with the fetal head at -1 station. The patient forgoes epidural anesthesia. During which of the following scenarios should a cesarean delivery be considered for this patient?
A 28-year-old primigravid woman at 36 weeks' gestation comes to the emergency department for 2 hours of contractions. Her pregnancy has been uncomplicated. The contractions occur once every 20–30 minutes, last less than 30 seconds, and have been consistent in intensity and duration since onset. During that time there has been an increase in fetal movements. Her temperature is 37.1°C (98.8°F), pulse is 98/min, and blood pressure is 104/76 mm Hg. Pelvic examination shows clear cervical mucus and a firm uterus consistent in size with a 36-week gestation. The cervix is 0% effaced and undilated; the vertex is at -3 station. The fetal heart rate is reassuring. After an hour of monitoring in the emergency department, the character of the contractions and pelvic examination findings remain unchanged. Which of the following is the most appropriate next step?
A 22-year-old primigravid woman at 41 weeks' gestation is admitted to the hospital in active labor. Pregnancy has been uncomplicated. She has asthma treated with theophylline and inhaled corticosteroids. She has had 2 surgeries in the past to repair multiple lower limb and pelvis fractures that were the result of a car accident. She is otherwise healthy. Her temperature is 37.2°C (99°F) and blood pressure is 108/70 mm Hg. Examination shows the cervix is 100% effaced and 10 cm dilated; the vertex is at -4 station, with the occiput in the anterior position. Uterine activity is measured at 275 MVUs. Maternal pushing occurs during the contractions. Fetal heart tracing is 166/min and reactive with no decelerations. Epidural anesthesia is initiated for pain relief. After 4 hours of pushing, the vertex is found to be at -4 station, with increasing strength and rate of uterine contractions; fetal heart tracing shows late decelerations. Which of the following is the most likely cause of this patient's prolonged labor?
A 62-year-old woman makes an appointment with her primary care physician because she recently started experiencing post-menopausal bleeding. She states that she suffered from anorexia as a young adult and has been thin throughout her life. She says that this nutritional deficit is likely what caused her to not experience menarche until age 15. She used oral contraceptive pills for many years, has never been pregnant, and experienced menopause at age 50. A biopsy of tissue inside the uterus reveals foci of both benign and malignant glandular cells. Which of the following was a risk factor for the development of the most likely cause of her symptoms?
A 27-year old primigravid woman at 37 weeks' gestation comes to the emergency department because of frequent contractions for 4 hours. Her pregnancy has been complicated by hyperemesis gravidarum which subsided in the second trimester. The contractions occur every 10–15 minutes and have been increasing in intensity and duration since onset. Her temperature is 37.1°C (98.8°F), pulse is 110/min, and blood pressure is 140/85 mm Hg. Uterine contractions are felt on palpation. Pelvic examination shows clear fluid in the vagina. The cervix is 50% effaced and 3 cm dilated. After 4 hours the cervix is 80% effaced and 6 cm dilated. Pelvic examination is inconclusive for the position of the fetal head. The fetal heart rate is reassuring. Which of the following is the most appropriate next step?
A 33-year-old woman, gravida 2, para 1, at 26 weeks' gestation comes to the emergency department because of frequent contractions. The contractions are 40 seconds each, occurring every 2 minutes, and increasing in intensity. Her first child was delivered by lower segment transverse cesarean section because of a nonreassuring fetal heart rate. Her current medications include folic acid and a multivitamin. Her temperature is 36.9°C (98.4°F), heart rate is 88/min, and blood pressure is 126/76 mm Hg. Contractions are felt on the abdomen. There is clear fluid in the vulva and the introitus. The cervix is dilated to 5 cm, 70% effaced, and station of the head is -2. A fetal ultrasound shows polyhydramnios, a median cleft lip, and fused thalami. The corpus callosum, 3rd ventricle, and lateral ventricles are absent. The spine shows no abnormalities and there is a four chamber heart. Which of the following is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app