
Augmentation of labor — MCQs

A 36-year-old primigravid woman at 26 weeks' gestation comes to the physician complaining of absent fetal movements for the last 2 days. Pregnancy was confirmed by ultrasonography 14 weeks earlier. She has no vaginal bleeding or discharge. She has a history of type 1 diabetes mellitus controlled with insulin. Vital signs are all within the normal limits. Pelvic examination shows a soft, 2-cm long cervix in the midline with a cervical os measuring 3 cm and a uterus consistent in size with 24 weeks' gestation. Transvaginal ultrasonography shows a fetus with no cardiac activity. Which of the following is the most appropriate next step in management?
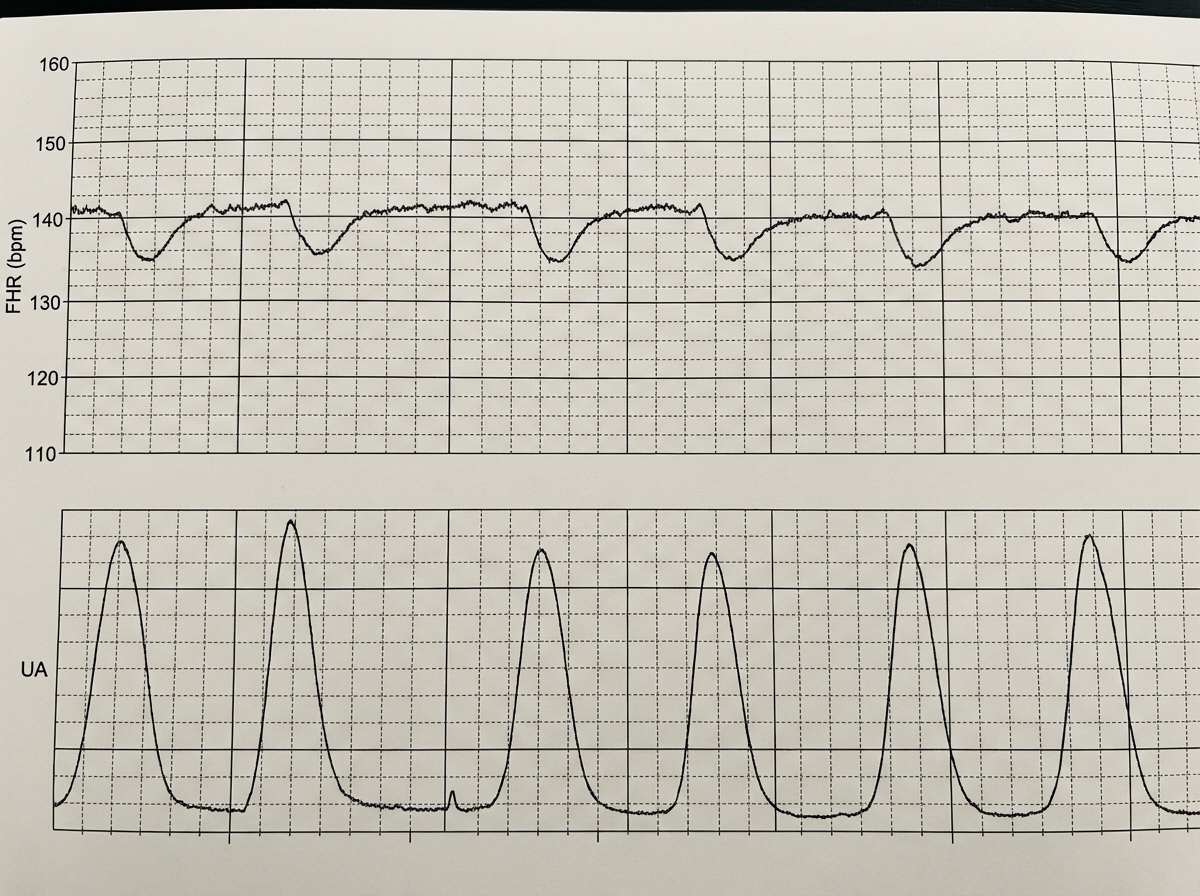
A 39-year-old woman, gravida 5, para 4, at 41 weeks' gestation is brought to the hospital because of regular uterine contractions that started 2 hours ago. Pregnancy has been complicated by iron deficiency anemia treated with iron supplements. Pelvic examination shows the cervix is 90% effaced and 7-cm dilated; the vertex is at -1 station. Fetal heart tracing is shown. The patient is repositioned, O2 therapy is initiated, and amnioinfusion is done. A repeat assessment after 20 minutes shows a similar cervical status, and no changes in the fetal heart tracing, and less than 5 contractions in a period of 10 minutes.What is the most appropriate next step in management?
A 22-year-old G4P2 at 35 weeks gestation presents to the hospital after she noticed that "her water broke." Her prenatal course is unremarkable, but her obstetric history includes postpartum hemorrhage after her third pregnancy, attributed to a retained placenta. The patient undergoes augmentation of labor with oxytocin and within four hours delivers a male infant with Apgar scores of 8 and 9 at 1 and 5 minutes, respectively. Three minutes later, the placenta passes the vagina, but a smooth mass attached to the placenta continues to follow. Her temperature is 98.6°F (37°C), blood pressure is 110/70 mmHg, pulse is 90/min, and respirations are 20/min. What is the most likely complication in the absence of intervention?
A 27-year old primigravid woman at 37 weeks' gestation comes to the emergency department because of frequent contractions for 4 hours. Her pregnancy has been complicated by hyperemesis gravidarum which subsided in the second trimester. The contractions occur every 10–15 minutes and have been increasing in intensity and duration since onset. Her temperature is 37.1°C (98.8°F), pulse is 110/min, and blood pressure is 140/85 mm Hg. Uterine contractions are felt on palpation. Pelvic examination shows clear fluid in the vagina. The cervix is 50% effaced and 3 cm dilated. After 4 hours the cervix is 80% effaced and 6 cm dilated. Pelvic examination is inconclusive for the position of the fetal head. The fetal heart rate is reassuring. Which of the following is the most appropriate next step?
You are a resident in the surgical ICU. One of the patients you are covering is a 35-year-old pregnant G1P0 in her first trimester admitted for complicated appendicitis and awaiting appendectomy. Your attending surgeon would like you to start the patient on moxifloxacin IV preoperatively. You remember from your obstetrics clerkship, however, that moxifloxacin is Pregnancy Category C, and animal studies have shown that immature animals exposed to fluoroquinolones like moxifloxacin may experience cartilage damage. You know that there are potentially safer antibiotics, such as piperacillin/tazobactam, which is in Pregnancy Category B. What should you do?
A 44-year-old woman with high blood pressure and diabetes presents to the outpatient clinic and informs you that she is trying to get pregnant. Her current medications include lisinopril, metformin, and sitagliptin. Her blood pressure is 136/92 mm Hg and heart rate is 79/min. Her physical examination is unremarkable. What should you do regarding her medication for high blood pressure?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 30-year-old woman, gravida 2, para 1, at 38 weeks' gestation comes to the hospital for regular, painful contractions that have been increasing in frequency. Her pregnancy has been complicated by gestational diabetes treated with insulin. Pelvic examination shows the cervix is 50% effaced and 4 cm dilated; the vertex is at -1 station. Ultrasonography shows no abnormalities. A tocometer and Doppler fetal heart monitor are placed on the patient's abdomen. The fetal heart rate monitoring strip shows a baseline heart rate of 145/min with a variability of ≥ 15/min. Within a 20-minute recording, there are 7 uterine contractions, 4 accelerations, and 3 decelerations that have a nadir occurring within half a minute. The decelerations occur at differing intervals relative to the contractions. Which of the following is the most appropriate next step in the management of this patient?
A 22-year-old primigravid woman at 41 weeks' gestation is admitted to the hospital in active labor. Pregnancy has been uncomplicated. She has asthma treated with theophylline and inhaled corticosteroids. She has had 2 surgeries in the past to repair multiple lower limb and pelvis fractures that were the result of a car accident. She is otherwise healthy. Her temperature is 37.2°C (99°F) and blood pressure is 108/70 mm Hg. Examination shows the cervix is 100% effaced and 10 cm dilated; the vertex is at -4 station, with the occiput in the anterior position. Uterine activity is measured at 275 MVUs. Maternal pushing occurs during the contractions. Fetal heart tracing is 166/min and reactive with no decelerations. Epidural anesthesia is initiated for pain relief. After 4 hours of pushing, the vertex is found to be at -4 station, with increasing strength and rate of uterine contractions; fetal heart tracing shows late decelerations. Which of the following is the most likely cause of this patient's prolonged labor?
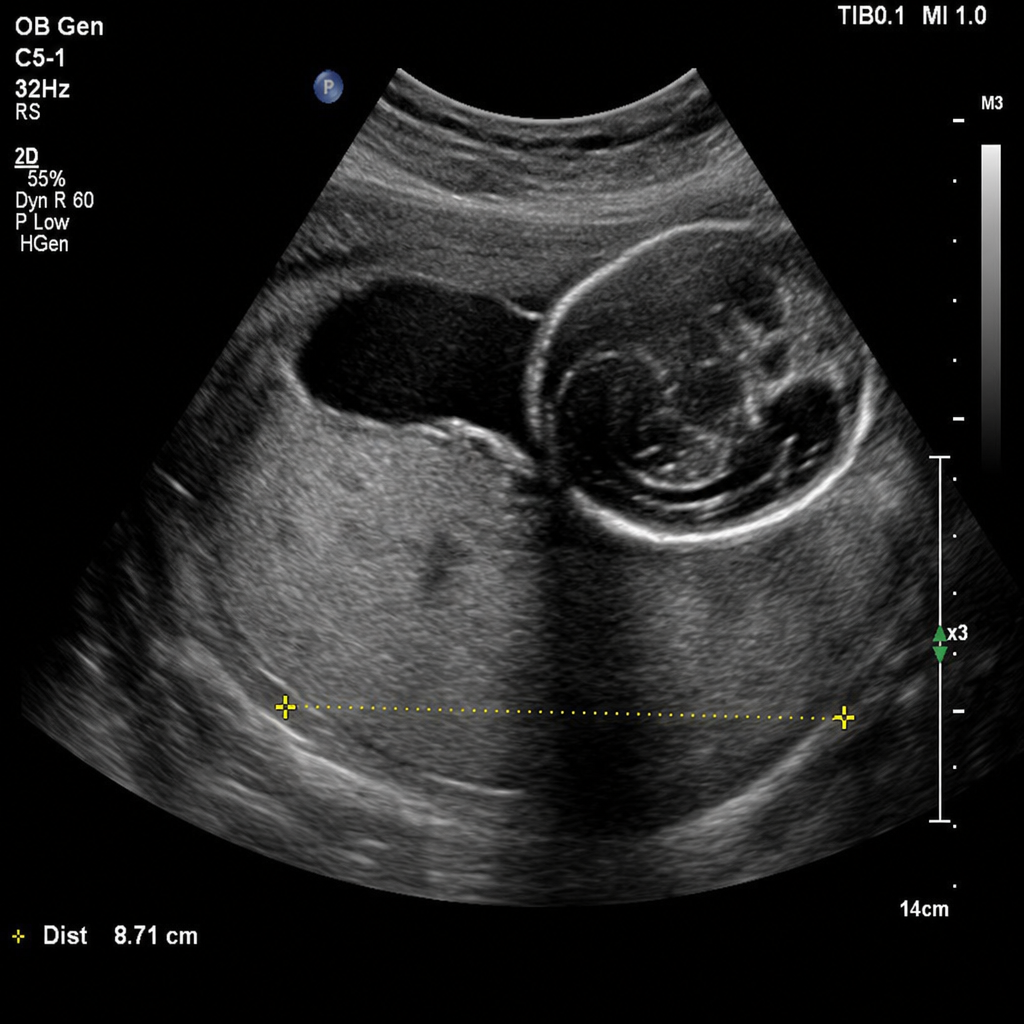
A 31-year-old woman, G3P2, at 32 weeks of gestation presents with a sudden onset of painless vaginal bleeding. She soaked two pads over the past hour. Vital signs: BP 110/70 mmHg, HR 96 bpm. The fetal heart rate tracing shows a baseline of 150 bpm with moderate variability, accelerations present, and no decelerations. A transabdominal ultrasound obtained at presentation demonstrates the placenta completely covering the internal os. Based on the ultrasound findings, which of the following is the most appropriate management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app