
Stages of labor — MCQs

On this page
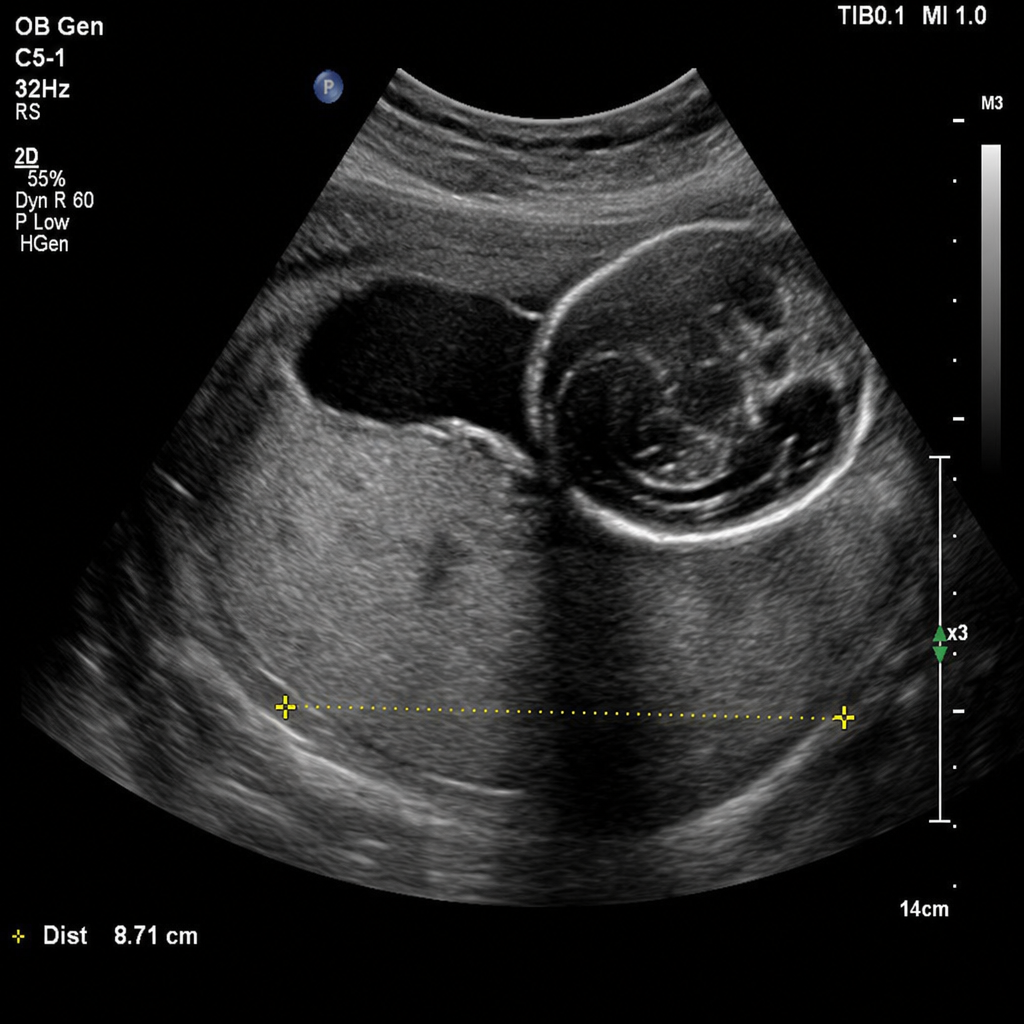
A 31-year-old woman, G3P2, at 32 weeks of gestation presents with a sudden onset of painless vaginal bleeding. She soaked two pads over the past hour. Vital signs: BP 110/70 mmHg, HR 96 bpm. The fetal heart rate tracing shows a baseline of 150 bpm with moderate variability, accelerations present, and no decelerations. A transabdominal ultrasound obtained at presentation demonstrates the placenta completely covering the internal os. Based on the ultrasound findings, which of the following is the most appropriate management?
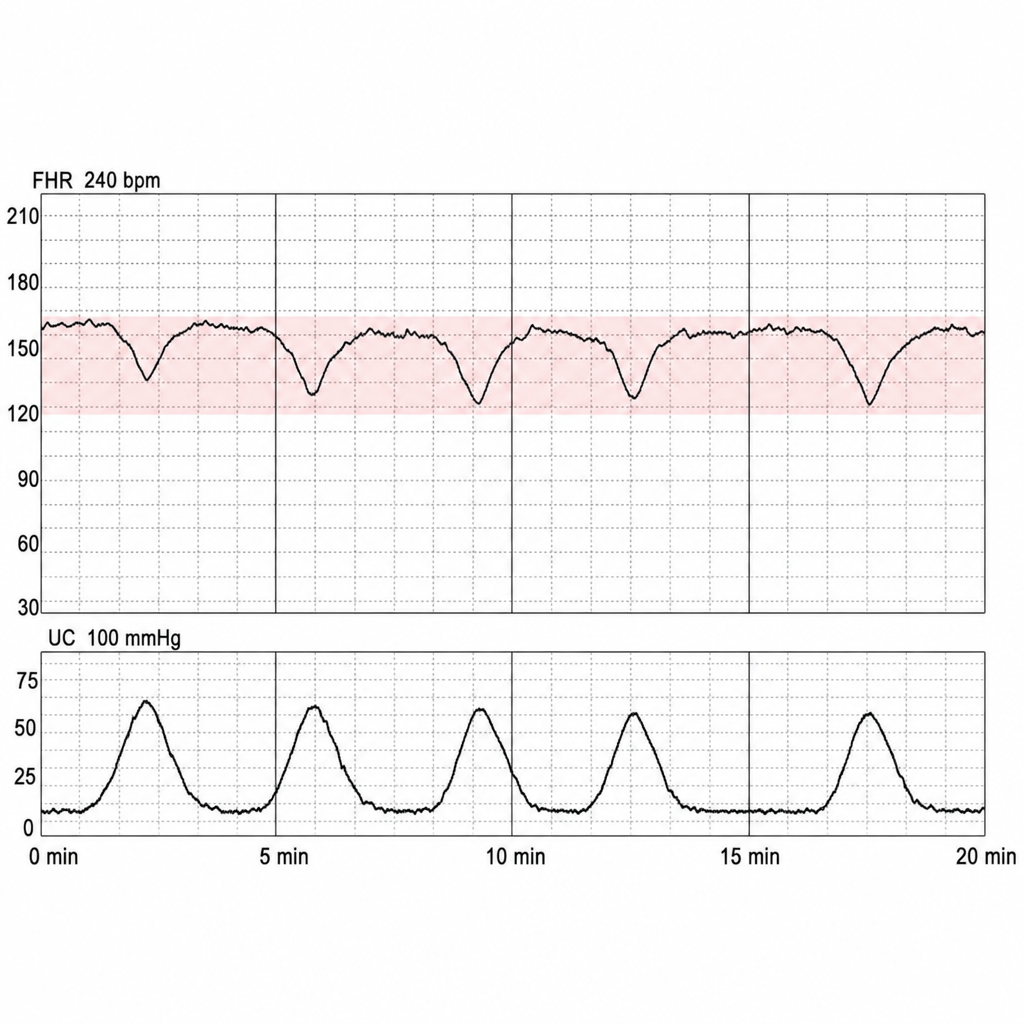
A 34-year-old woman, G2P1, at 39 weeks of gestation is in active labor. Her prior delivery was by cesarean for breech presentation. She desires a trial of labor after cesarean. She is 7 cm dilated and contractions are every 3 minutes. Fetal heart rate monitoring over the past 20 minutes shows a baseline of 160 bpm, absent variability, no accelerations, and repetitive late decelerations with each contraction. Oxygen is applied by face mask and the patient is repositioned to the left lateral decubitus position. Repeat tracing 10 minutes later is unchanged. IV fluid bolus is administered. Which of the following is the most appropriate next step?
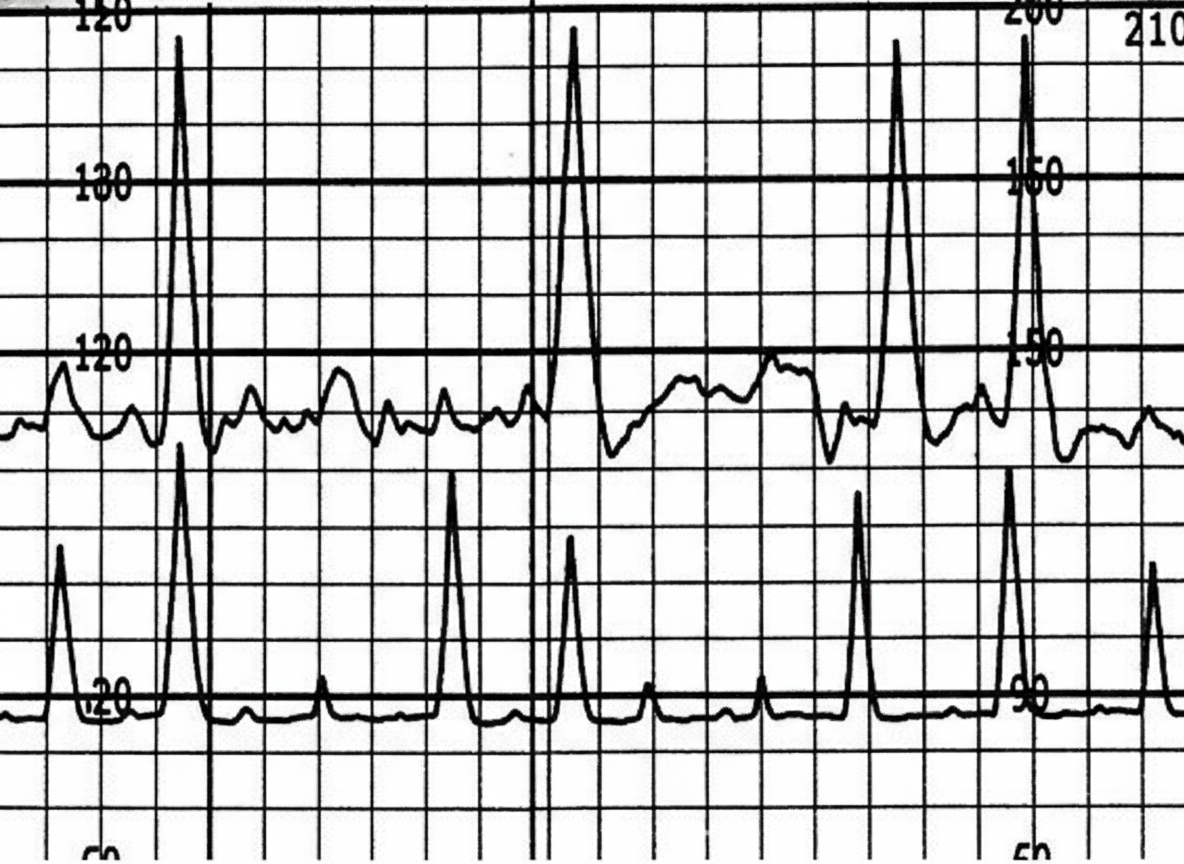
A 28-year-old woman, gravida 2, para 1, at 40 weeks of gestation is admitted to the hospital in active labor. The patient has attended many prenatal appointments and followed her physician's advice about screening for diseases, laboratory testing, diet, and exercise. Her pregnancy has been uncomplicated. She has no history of a serious illness. Her first child was delivered via normal vaginal delivery. Her vital signs are within normal limits. Cervical examination shows 80% effacement, 5 cm dilation and softening without visible fetal parts or prolapsed umbilical cord. A cardiotocograph is shown. Which of the following options is the most appropriate initial step in management?
A 23-year-old woman presents to her gynecologist for painful menses. Her menses are regular, occurring every 28 days and lasting approximately 4 days. Menarche was at age 12. Over the past 6 months, she has started to develop aching pelvic pain during the first 2 days of her menstrual period. Ibuprofen provides moderate relief of her symptoms. She denies nausea, vomiting, dyschezia, dyspareunia, irregular menses, or menses that are heavier than usual. Her past medical history is notable for chlamydia 4 years ago that was treated appropriately. She currently takes no medications. She works as a copywriter and does not smoke or drink. She has been in a monogamous relationship with her boyfriend for the past 3 years. They use condoms intermittently. Her temperature is 98.6°F (37°C), blood pressure is 111/69 mmHg, pulse is 92/min, and respirations are 18/min. Pelvic examination demonstrates a normal appearing vagina with no adnexal or cervical motion tenderness. The uterus is flexible and anteverted. Which of the following is the underlying cause of this patient's pain?
A 26-year-old gravida 1 at 36 weeks gestation is brought to the emergency department by her husband complaining of contractions lasting up to 2 minutes. The contractions are mostly in the front of her abdomen and do not radiate. The frequency and intensity of contractions have not changed since the onset. The patient worries that she is in labor. The blood pressure is 125/80 mm Hg, the heart rate is 96/min, the respiratory rate is 15/min, and the temperature 36.8°C (98.2℉). The physical examination is unremarkable. The estimated fetal weight is 3200 g (6.6 lb). The fetal heart rate is 146/min. The cervix is not dilated. The vertex is at the -4 station. Which of the following would be proper short-term management of this woman?
Practice by Chapter
Physiology of parturition
Practice Questions
First stage of labor
Practice Questions
Second stage of labor
Practice Questions
Third stage of labor
Practice Questions
Fourth stage of labor
Practice Questions
Cardinal movements of labor
Practice Questions
Labor curve and Friedman curve
Practice Questions
Induction of labor indications and methods
Practice Questions
Augmentation of labor
Practice Questions
Cervical ripening methods
Practice Questions
Fetal heart rate monitoring
Practice Questions
Pain management in labor
Practice Questions
Operative vaginal delivery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app