
Screening tests — MCQs

On this page
A 32-year-old nulligravid woman comes to the physician because of 2 weeks of postcoital pain and blood-tinged vaginal discharge. She has been sexually active with one male partner for the past 3 months. They do not use condoms. Her only medication is a combined oral contraceptive that she has been taking for the past 2 years. She states that she takes the medication fairly consistently, but may forget a pill 2–3 days per month. One year ago, her Pap smear was normal. She has not received the HPV vaccine. The cervix is tender to motion on bimanual exam. There is bleeding when the cervix is touched with a cotton swab during speculum exam. Which of the following is the most likely diagnosis?
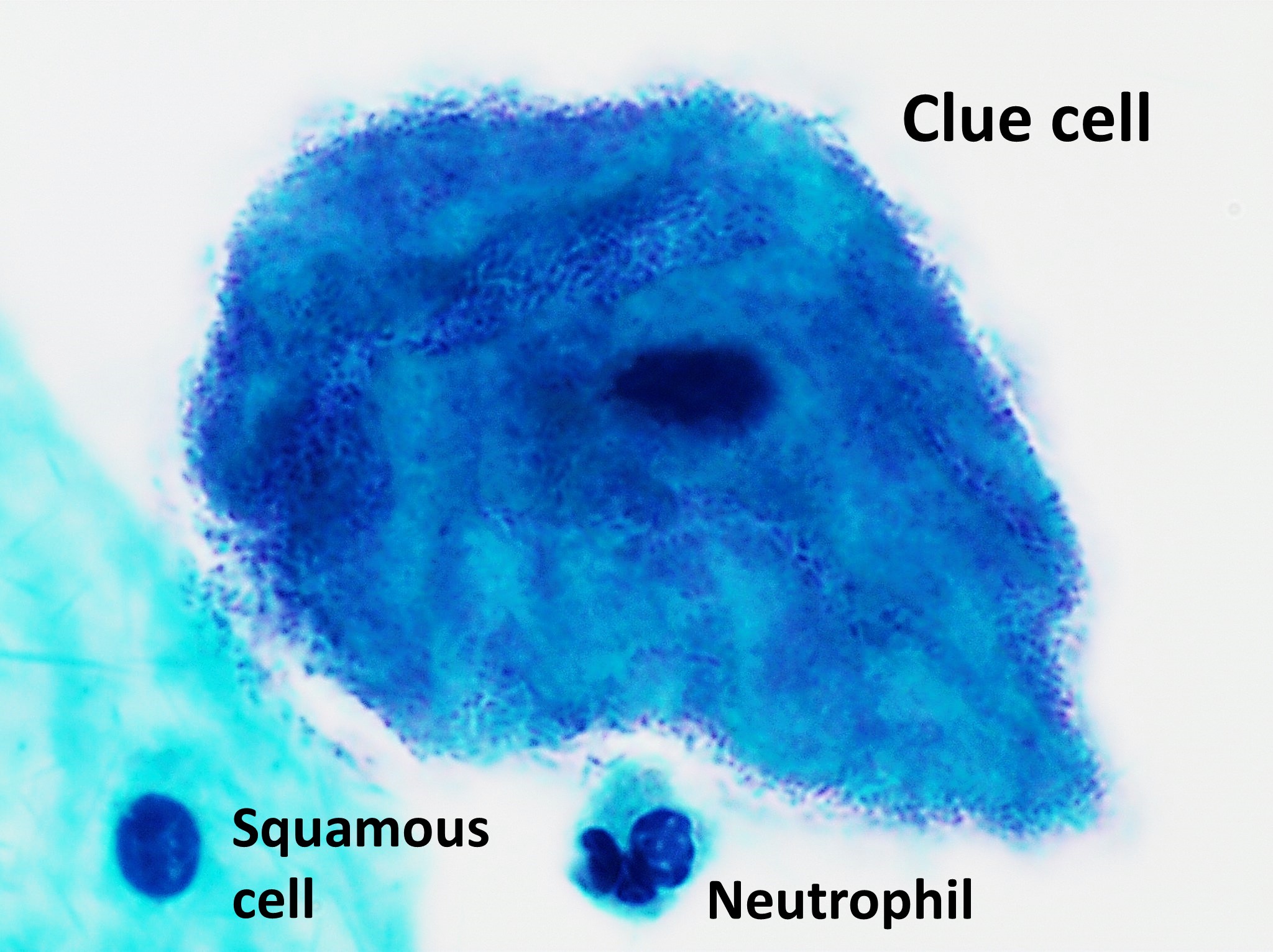
A 22-year-old woman presents to her physician with an increased vaginal discharge. She has no other complaints. She has recently changed her sexual partner, who claims to have no genitourinary symptoms. They do not use condoms. Her vital signs are as follows: blood pressure, 110/80 mm Hg; heart rate, 65/min; respiratory rate, 11/min; and temperature, 36.6℃ (97.9℉). Her physical examination is unremarkable. The gynecologic examination shows increased production of a white-yellow vaginal discharge. Wet mount microscopy shows the below picture. Which of the following treatments is indicated in this patient?
A 22-year-old woman presents to an outpatient clinic complaining of an increasing vaginal discharge over the last week. The discharge is foul-smelling. The menstrual cycles are regular and last 4–5 days. The patient denies postcoital or intermenstrual bleeding. The last menstrual period was 2 weeks ago. She mentions that she has been sexually active with 2 new partners for the past 2 months, but they use condoms inconsistently. The patient has no chronic conditions, no previous surgeries, and does not take any medications. She is afebrile. The blood pressure is 125/82 mm Hg, the pulse is 102/min, and the respiratory rate is 19/min. The physical examination reveals a thin, yellow-green discharge accompanied by a pink and edematous vagina and a red-tan cervix. Which of the following is the most likely diagnosis?
A 21-year-old woman comes to the physician because of multiple painful, purulent ulcers she noticed on her vulva 2 days ago. The patient has not had fever or burning with urination. She has no history of similar lesions. She had a chlamydial infection at 17 years of age that was treated with antibiotics. Her immunizations are up-to-date. She is sexually active with her boyfriend of 2 months and uses an oral contraceptive; they use condoms inconsistently. Her temperature is 37.2°C (99.0°F), pulse is 94/min, and blood pressure is 120/76 mm Hg. Examination shows tender inguinal lymphadenopathy. There are 4 tender, purulent 1.5-cm ulcers with a necrotic base along the labia majora. Which of the following is the most likely diagnosis?
A 37-year-old woman comes for a follow-up prenatal visit at 18 weeks' gestation. At 12 weeks' gestation, ultrasonography showed increased nuchal translucency and pregnancy-associated plasma protein A (PAPP-A) was decreased by 2 standard deviations. Chorionic villus sampling showed a 47, XX, +21 karyotype. During this visit, ultrasonography shows a hypoplastic nasal bone, shortened femur length, shortened middle phalanges of the fifth digits with clinodactyly. A quadruple marker test would most likely show which of the following sets of findings? $$$ α-Fetoprotein (AFP) %%% Estriol %%% β-Human chorionic gonadotropin (HCG) %%% Inhibin A $$$
A 32-year-old woman, gravida 2, para 2, comes to the physician for the evaluation of a palpable mass in her right breast that she first noticed 1 week ago. She has no associated pain. She has never had a mammogram previously. She has type II diabetes mellitus treated with metformin. She has no family history of breast cancer. She has smoked half a pack of cigarettes daily for 15 years. Her temperature is 37°C (98.6°F), pulse is 78/min, respirations are 14/min, and blood pressure is 125/75 mm Hg. Examination shows a firm, nonpainful, nonmobile mass in the right upper quadrant of the breast. There is no nipple discharge. Examination of the skin and lymph nodes shows no abnormalities. No masses are palpated in the left breast. Which of the following is the most appropriate next step in the management of this patient?
A 24-year-old woman comes to the physician for a routine pelvic examination. She feels well. Menses occur at 30-day intervals and last 7 days. Her last menstrual period was 6 days ago. She has no history of abnormal Pap smears; her last Pap smear was 13 months ago. She is sexually active with three male partners and uses condoms consistently. She has never been tested for sexually transmitted infections. Her 54-year-old mother has breast cancer. She is up-to-date on her Tdap, MMR, and varicella vaccinations. Her temperature is 37.1°C (98.8°F), pulse is 68/min, and blood pressure is 108/68 mm Hg. Physical examination shows no abnormalities. In addition to HIV, gonorrhea, and chlamydia testing, which of the following is the most appropriate recommendation at this time?
A 28-year-old G2P1 female is concerned that she may give birth to another child with Down syndrome. She states that she may not be able to take care of another child with this disorder. Which of the following tests can confirm the diagnosis of Down syndrome in utero?
A 41-year-old woman comes to the physician because of bleeding from the nipple of her right breast for 3 months. There is no bleeding from the other breast. Menses occur at regular 30-day intervals and lasts for 5 days with moderate flow. Her last menstrual period was 1 week ago. Her mother died of breast cancer at the age of 53 years. She does not smoke or drink alcohol. She appears healthy. Her temperature is 37°C (98.7°F), pulse is 76/min, and blood pressure is 118/70 mm Hg. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and nontender. Breast examination shows bleeding of the right breast on application of pressure with no palpable mass. The left breast shows no abnormalities. There is no palpable axillary lymphadenopathy. Pelvic examination shows a normal vagina and cervix. Ultrasonography shows a dilated duct enclosing a well-defined solitary mass. Which of the following is the most likely diagnosis?
A 57-year-old nulliparous woman comes to the physician 2 weeks after noticing a lump in her right breast. Her last mammogram was performed 4 years ago and showed no abnormalities. Menopause began 2 years ago, during which time the patient was prescribed hormone replacement therapy for severe hot flashes and vaginal dryness. Vital signs are within normal limits. Examination of the right breast shows a firm, nontender mass close to the nipple. There are no changes in the skin or nipple, and there is no palpable axillary adenopathy. The abdomen is soft and nontender; there is no organomegaly. Mammography shows a suspicious 2-cm mass adjacent to the nipple. Which of the following is the most appropriate next step in management?
Practice by Chapter
First trimester screening
Practice Questions
Cell-free DNA screening
Practice Questions
Second trimester serum screening
Practice Questions
Ultrasound markers and anomaly screening
Practice Questions
Carrier screening for genetic disorders
Practice Questions
Cervical cancer screening in pregnancy
Practice Questions
Diabetes screening in pregnancy
Practice Questions
Gestational diabetes management
Practice Questions
Group B streptococcus screening
Practice Questions
Screening for preeclampsia risk factors
Practice Questions
Prenatal infection screening (TORCH, HIV, STIs)
Practice Questions
Genetic counseling principles
Practice Questions
Diagnostic testing (amniocentesis, CVS)
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app