
Screening tests — MCQs

On this page
A 52-year-old woman visits your office complaining about discharge from her left nipple for the past 3 months. The discharge looks like gray greenish and its amount is progressively increasing. She appears to be anxious and extremely uncomfortable with this situation as it is embarrassing for her when it occurs outdoors. Past medical history is insignificant. Her family history is negative for breast and ovarian disorders. She tries to stay active by running for 30 minutes every day on a treadmill, staying away from smoking, and by eating a balanced diet. She drinks alcohol occasionally. During physical examination you find a firm, stable mass under an inverted nipple in her left breast; while on the right breast, dilated subareolar ducts can be noted. There is no lymphadenopathy and remaining of the physical exam is normal. A mammogram is performed which reveals tubular calcifications. Which of the following is the most likely diagnosis?
A 24-year-old gravida 2 para 0 presents to her physician at 15 weeks gestation to discuss the results of recent screening tests. She has no complaints and the current pregnancy has been uncomplicated. Her previous pregnancy terminated with spontaneous abortion in the first trimester. Her immunizations are up to date. Her vital signs are as follows: blood pressure 110/60 mm Hg, heart rate 78/min, respiratory rate 14/min, and temperature 36.8℃ (98.2℉). The physical examination is within normal limits. The laboratory screening tests show the following results: HBsAg negative HBcAg negative Anti-HBsAg positive HIV 1/2 AB negative VDRL positive What is the proper next step in the management of this patient?
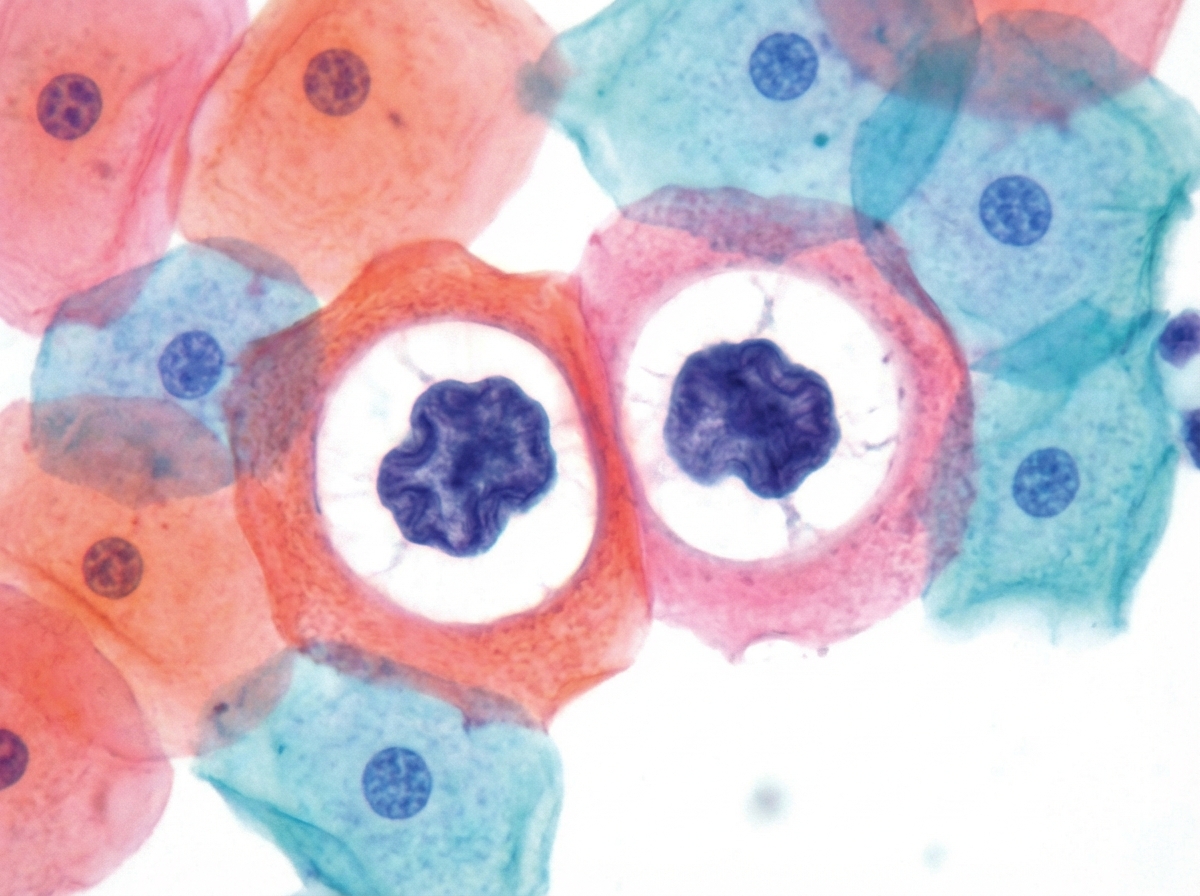
A 36-year-old woman comes to the physician for an annual pelvic examination and Pap smear. Her last Pap smear was 3 years ago. She has been sexually active with multiple male partners and takes an oral contraceptive. She has smoked one pack of cigarettes daily for 10 years. Pelvic examination shows no abnormalities. A photomicrograph of cervical cells from the Pap smear specimen is shown. Cells similar to the one indicated by the arrow are most likely to be seen in which of the following conditions?
A 32-year-old woman presented for her annual physical examination. She mentioned that her family history had changed since her last visit: her mother was recently diagnosed with breast cancer and her sister tested positive for the BRCA2 mutation. The patient, therefore, requested testing as well. If the patient tests positive for the BRCA1 or BRCA2 mutation, which of the following is the best screening approach?
A 62-year-old woman presents to her primary care physician for a routine physical exam. The patient has no specific complaints but does comment on some mild weight gain. She reports that she recently retired from her job as a math teacher and has taken up hiking. Despite the increase in activity, she believes her pants have become "tighter." She denies headaches, urinary symptoms, or joint pains. She has a history of hypertension, type 2 diabetes, and rheumatoid arthritis. Her medications include aspirin, lisinopril, rovastatin, metformin, and methotrexate. She takes her medications as prescribed and is up to date with her vaccinations. A colonoscopy two years ago and a routine mammography last year were both normal. The patient’s last menstrual period was 10 years ago. The patient has a father who died of colon cancer at 71 years of age and a mother who has breast cancer. Her temperature is 98.7°F (37°C), blood pressure is 132/86 mmHg, pulse is 86/min, respirations are 14/min and oxygen saturation is 98% on room air. Physical exam is notable for a mildly distended abdomen and a firm and non-mobile right adnexal mass. What is the next step in the management of this patient?
A 36-year-old G4P0A3 woman presents at the prenatal diagnostic center at 18 weeks of gestation for the scheduled fetal anomaly scan. The patient's past medical history reveals spontaneous abortions. She reports that her 1st, 2nd, and 3rd pregnancy losses occurred at 8, 10, and 12 weeks of gestation, respectively. Ultrasonography indicates a female fetus with cystic hygroma (measuring 4 cm x 5 cm in size) and fetal hydrops. Which of the following karyotypes does her fetus most likely carry?
A 23-year-old woman presents to the emergency department with abnormal vaginal discharge and itchiness. She states it started a few days ago and has been worsening. The patient has a past medical history of a medical abortion completed 1 year ago. Her temperature is 98.6°F (37.0°C), blood pressure is 129/68 mmHg, pulse is 80/min, respirations are 14/min, and oxygen saturation is 99% on room air. Physical exam demonstrates an anxious woman. Pelvic exam reveals yellow cervical discharge. Nucleic acid amplification test is negative for Neisseria species. Which of the following is the best next step in management?
A 34-year-old G2P2 undergoes colposcopy due to high-grade intraepithelial neoplasia detected on a Pap smear. Her 2 previous Pap smears showed low-grade intraepithelial neoplasia. She has had 2 sexual partners in her life, and her husband has been her only sexual partner for the last 10 years. She had her sexual debut at 16 years of age. She had her first pregnancy at 26 years of age. She uses oral contraceptives for birth control. Her medical history is significant for right ovary resection due to a large follicular cyst and cocaine abuse for which she completed a rehabilitation program. Colposcopy reveals an acetowhite lesion with distorted vascularity at 4 o'clock. Which of the following factors present in this patient is a risk factor for the detected condition?
A 23-year-old pregnant woman (gravida 1, para 0) presents during her 16th week of pregnancy for a check-up. The course of her current pregnancy is unremarkable. She had normal results on the previous ultrasound examination. Her human chorionic gonadotropin (hCG) level measured at week 12 of pregnancy was 0.9 multiples of the normal median (MoM). She is human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV)-negative. She undergoes a quadruple test which shows the following results: Serum alpha-fetoprotein Low Unconjugated estriol Low Beta-hCG High Inhibin A High The risk of which condition indicates these results?
A 39-year-old woman comes to the physician because of a 6-month history of vaginal bleeding for 2 to 5 days every 2 to 3 weeks. The flow is heavy with passage of clots. Menarche occurred at the age of 10 years, and menses previously occurred at regular 28- to 32- day intervals and lasted for 5 days with normal flow. Her only medication is a multivitamin. She has no children. Her mother was diagnosed with ovarian cancer at age 60. She is 158 cm (5 ft 2 in) tall and weighs 86 kg (190 lb); BMI is 34 kg/m2. Her temperature is 36.6°C (97.8°F), pulse is 86/min and blood pressure is 110/70 mm Hg. Pelvic examination shows a normal sized uterus. Laboratory studies, including a complete blood count, thyroid function tests, and coagulation studies are within the reference ranges. A urine pregnancy test is negative. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
Practice by Chapter
First trimester screening
Practice Questions
Cell-free DNA screening
Practice Questions
Second trimester serum screening
Practice Questions
Ultrasound markers and anomaly screening
Practice Questions
Carrier screening for genetic disorders
Practice Questions
Cervical cancer screening in pregnancy
Practice Questions
Diabetes screening in pregnancy
Practice Questions
Gestational diabetes management
Practice Questions
Group B streptococcus screening
Practice Questions
Screening for preeclampsia risk factors
Practice Questions
Prenatal infection screening (TORCH, HIV, STIs)
Practice Questions
Genetic counseling principles
Practice Questions
Diagnostic testing (amniocentesis, CVS)
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app