
Screening tests — MCQs

On this page
A 29-year-old woman presents to her gynecologist because of chronic pelvic pain that she has been experiencing for the last 6 months. Specifically, she says that she has severe pain during menstruation that is localized primarily to her lower abdomen and pelvis. In addition, she has been having pain while defecating and during intercourse. She has no past surgical history and her past medical history is significant for asthma. She uses protection while having intercourse with her long time boyfriend and has never been pregnant. Physical exam reveals adnexal tenderness and the presence of an adnexal mass. Laparoscopic examination is conducted showing several cysts filled with dark brown fluid on her ovaries and powder burn marks along her peritoneal surfaces. Which of the following markers would most likely be elevated in this patient?
A 29-year-old woman comes to the physician for evaluation of a mass in the left breast that she first noticed 2 weeks ago. During this period, the mass has not increased in size and the patient has had no pain. Three months ago, she hit her left chest against the closet door, which was painful for a day. Menses occurs at regular 28-day intervals and last for 5 days with moderate flow. Her last menstrual period was 3 weeks ago. Physical examination shows dense breasts and a 2.5-cm well-defined, rubbery, mobile mass that is nontender in the upper outer quadrant of the left breast. There is no axillary adenopathy. Which of the following is the most likely diagnosis?
A 22-year-old Caucasian G1 presents to her physician at 29 weeks gestation for a checkup. The medical history is unremarkable and the current pregnancy has been uncomplicated. Her weight is 81 kg (178.6 lb) and the height is 169 cm (5 ft 6 in). She has gained 13 kg (28.6 lb) during the pregnancy. She has no abnormalities on physical examination. Which of the following screening tests should be obtained ?
A 36-year-old female presents to her gynecologist for a check-up. She has had normal Pap smears as recommended every 3 years since she turned 30 years old. The physician conducts a pelvic examination that is without abnormality and obtains a cervical Pap smear. The results of the patient's Pap smear from the visit return as high grade squamous intraepithelial lesion (HGSIL). Which of the following is the best next step in the management of this patient?
A 59-year-old woman comes to the physician because of worsening shortness of breath for the past two weeks. Physical examination shows decreased breath sounds at both lung bases. The abdomen is distended and there is shifting dullness with a positive fluid wave. Ultrasound of the abdomen shows a large collection of peritoneal fluid and a hypoechoic mass involving the left ovary. Microscopic examination of a biopsy specimen from the ovarian mass shows clusters of spindle-shaped cells. Which of the following is the most likely diagnosis?
A 17-year-old girl comes to the physician for an annual health maintenance examination. She feels well. She has no history of serious illness and her only medication is an oral contraceptive. Her mother was diagnosed with breast cancer at the age of 42 years. She is currently sexually active with 1 male partner and uses condoms inconsistently. Her immunizations are up-to-date. Her vital signs are within normal limits. Physical and pelvic examinations shows no abnormalities. An HIV test is negative. Which of the following is the most appropriate next step in management?
A 25-year-old woman comes to the physician for a routine health maintenance examination. Her last visit was 3 years ago. She feels well. One year ago, she underwent a tubectomy after the delivery of her third child. She does not take any medications. Physical examination shows no abnormalities. A Pap smear shows a high-grade squamous intraepithelial lesion. Which of the following is the most appropriate next step in management?
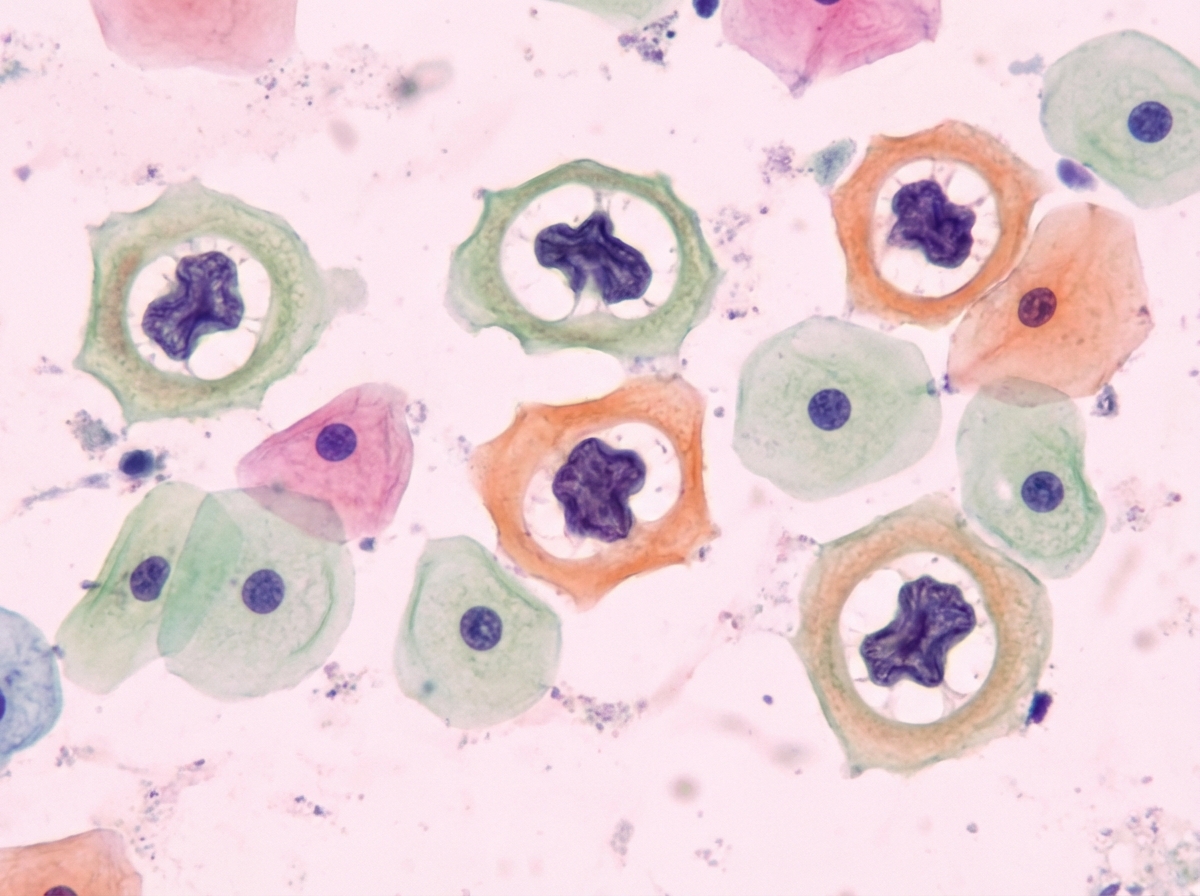
A 29-year-old woman presents to her gynecologist as part of her follow-up for her abnormal pap test a year ago. She has a normal menstrual cycle and has never been pregnant. She does not take oral contraceptive pills, as she is sexually inactive. She denies the use of any illicit drugs. Conventional cytology from her cervix uteri is done, which reveals pathological findings suggestive of a low-grade squamous intraepithelial lesion as shown in the photograph below. The same test last year revealed normal histological findings. What is the most likely process leading to these pathological findings in this patient’s pap smear?
A 16-year-old girl is brought to the physician by her mother because she has not attained menarche. She has no history of serious illness. She is at 50th percentile for height and weight. Examination shows no breast glandular tissue and no pubic hair development. The remainder of the examination shows no abnormalities. A urine pregnancy test is negative. An ultrasound of the pelvis shows no abnormalities. Which of the following is the most appropriate next step in management?
A 23-year-old woman presents to your office for a gynecological exam. She says that she has been in good health and has no complaints. She has been in a steady monogamous relationship for the past year. Physical examination was unremarkable. Screening tests are performed and return positive for gonorrhea. You treat her with an intramuscular injection of ceftriaxone and 7 day course of doxycycline. What else is recommended for this case?
Practice by Chapter
First trimester screening
Practice Questions
Cell-free DNA screening
Practice Questions
Second trimester serum screening
Practice Questions
Ultrasound markers and anomaly screening
Practice Questions
Carrier screening for genetic disorders
Practice Questions
Cervical cancer screening in pregnancy
Practice Questions
Diabetes screening in pregnancy
Practice Questions
Gestational diabetes management
Practice Questions
Group B streptococcus screening
Practice Questions
Screening for preeclampsia risk factors
Practice Questions
Prenatal infection screening (TORCH, HIV, STIs)
Practice Questions
Genetic counseling principles
Practice Questions
Diagnostic testing (amniocentesis, CVS)
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app