
Screening tests — MCQs

On this page
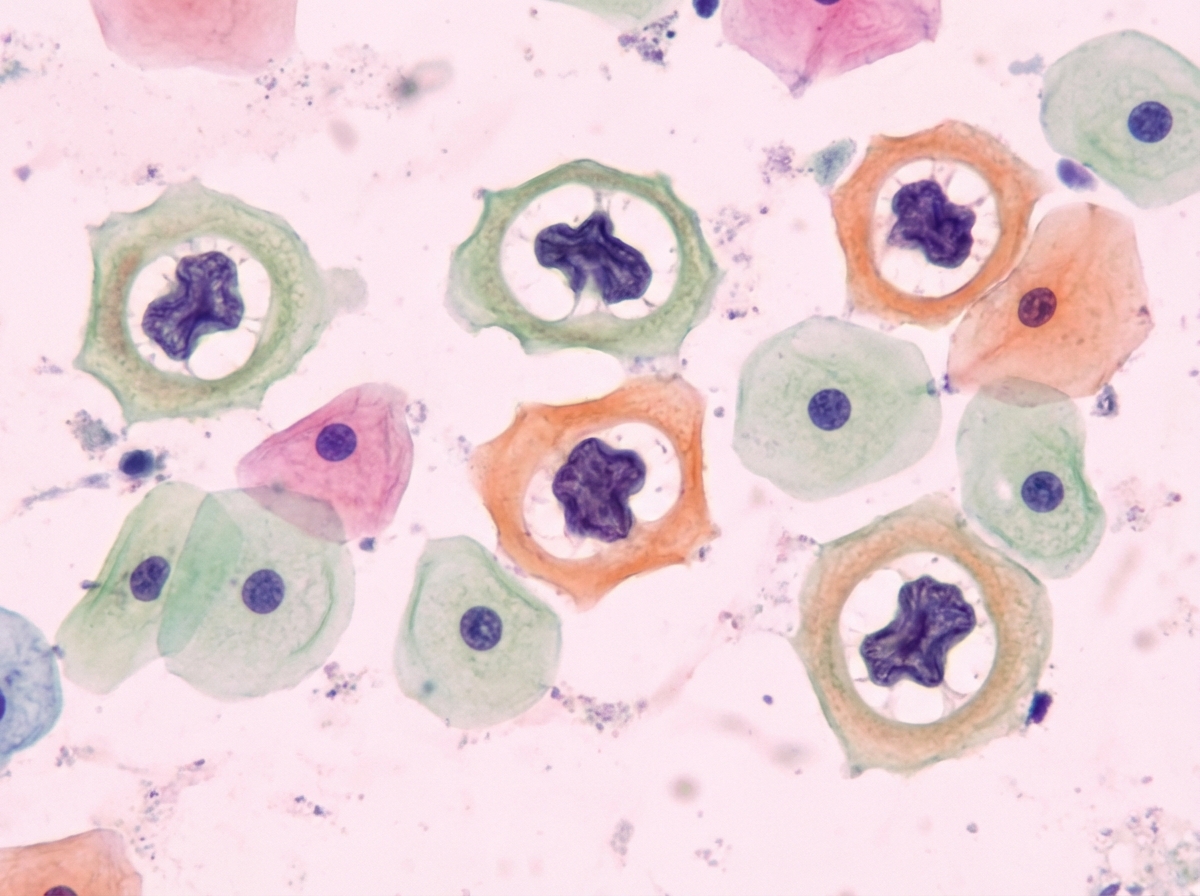
A 31-year-old woman presents to her gynecologist for a routine well-visit. She is sexually active with multiple male partners and uses an intrauterine device for contraception. Her last menstrual period was two weeks ago. She denies abnormal vaginal discharge or sensations of burning or itching. Pelvic exam is normal. Routine Pap smear shows the following (see Image A). Which organism is most likely responsible for her abnormal Pap smear?
A 27-year-old primigravida presents at 16 weeks gestation for a check-up. She has no co-existing diseases. Currently, she has no subjective complaints, but she worries about the results of her triple screen. She takes 400 mg of folic acid and 30 mg of iron daily. The results of the triple screen are shown below. Measured values Reference values Maternal serum alpha-fetoprotein 2.9 MoM 0.85-2.5 MoM Beta-hCG 1.1 MoM 0.5-1 MoM Unconjugated estriol 1 MoM 0.5-3 MoM What would be the most proper next step in the management of this patient?
A 24-year-old sexually active man complains of painless growths on his penis. He is worried that he might have transmitted them to his girlfriend. Biopsy shows squamous cells with perinuclear cytoplasmic vacuolization, nuclear enlargement, and koilocytes. The doctor treats the patient by treating the warts with cryoablation. The patient encourages his girlfriend to get tested too, as he is worried she is at increased risk of developing a malignancy. Which cancer is the patient worried about?
A 24-year-old woman presents to the emergency department with severe abdominal and lower back pain. She describes it as intense cramping and states that she experienced severe pain roughly 1 month ago that was similar. The patient's past medical history is non-contributory, and she states that her menses cause her to soak through 1 pad in a day. She is currently sexually active and does not use any contraception. Her vitals are within normal limits. The patient's abdominal exam is non-focal, and her pelvic exam reveals no adnexal masses or tenderness and no cervical motion tenderness. Which of the following is the most likely diagnosis?
A 28-year-old woman presents to discuss the results of her Pap smear. Her previous Pap smear 1 year ago showed atypical squamous cells of undetermined significance. This year the Pap smear was negative. She had a single pregnancy with a cesarean delivery. Currently, she and her partner do not use contraception because they are planning another pregnancy. She does not have any concurrent diseases and her family history is unremarkable. The patient is concerned about her previous Pap smear finding. She heard from her friend about a vaccine which can protect her against cervical cancer. She has never had such a vaccine and would like to be vaccinated. Which of the following answers regarding the vaccination in this patient is correct?
A 25-year-old nulliparous woman at 8 weeks' gestation comes to her physician accompanied by her husband for her first prenatal visit. She has no personal or family history of serious illness. Her vaccinations are up-to-date and she takes no medications. She has no history of recreational drug use and does not drink alcohol. Her vital signs are within normal limits. She is 167 cm (5 ft 6 in) tall and weighs 68 kg (150 lb); BMI is 24.3 kg/m2. She tested negative for HIV, Chlamydia trachomatis, and Neisseria gonorrhoeae 4 years ago. Which of the following tests should be done at this visit?
A 24-year-old woman at 6 weeks gestation seeks evaluation at a local walk-in clinic because she has noticed a clear, sticky discharge from her right nipple for the past 1 week. The discharge leaves a pink stain on her bra. She does not have pain in her breasts and denies changes in skin color or nipple shape. The past medical history is significant for a major depressive disorder, for which she takes fluoxetine. The family history is negative for breast, endometrial, and ovarian cancers. The physical examination is unremarkable. There are no palpable masses or tenderness on breast exam and no skin discoloration or ulcers. The breasts are symmetric. The nipple discharge on the right side is a pink secretion that is sticky. There are no secretions on the left. The axillary lymph nodes are normal. Which of the following is the most likely diagnosis?
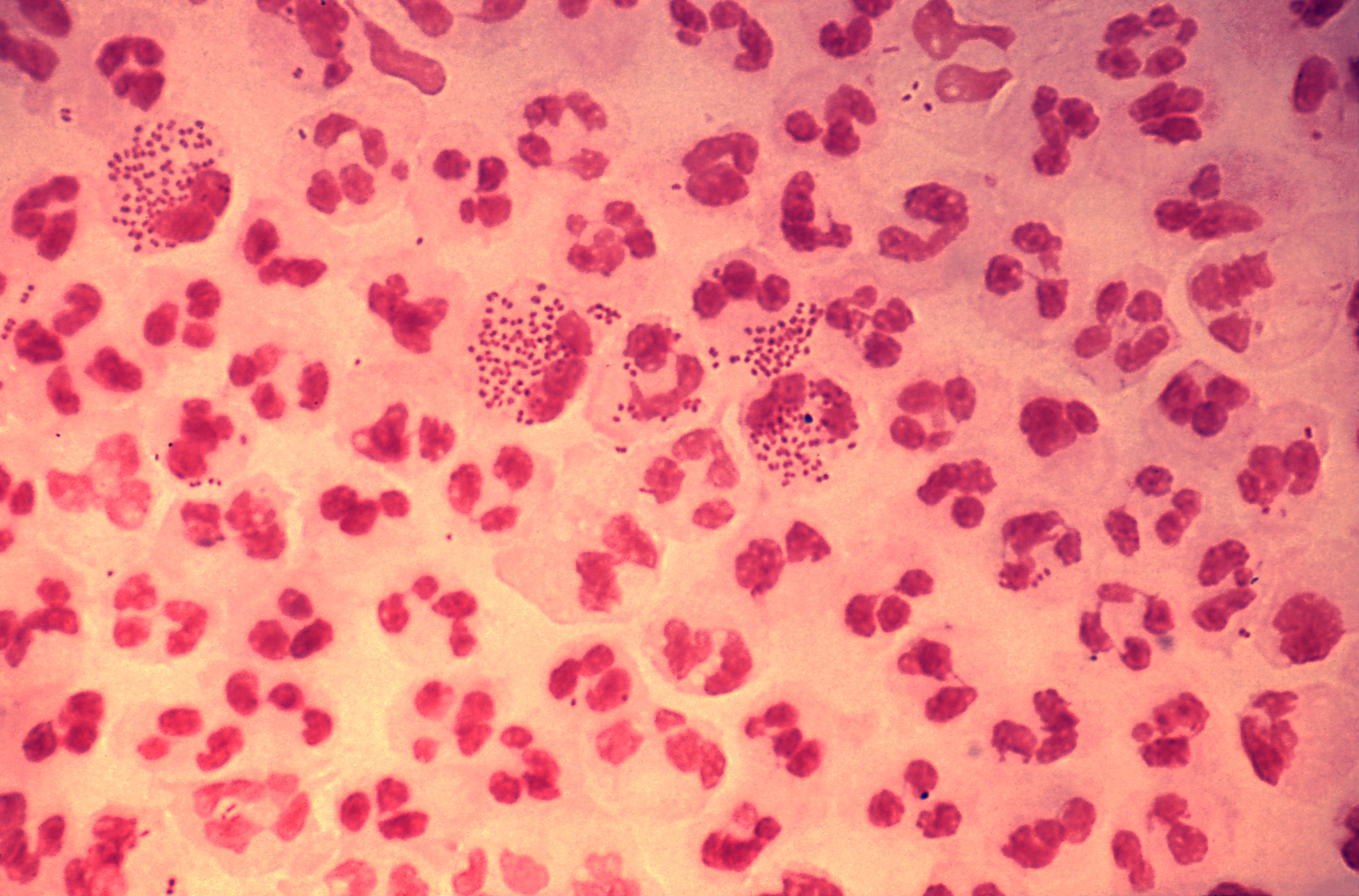
A 23-year-old woman comes to the physician because of vaginal discharge for 4 days. Her last menstrual period was 3 weeks ago. Twelve months ago, she was diagnosed with trichomoniasis, for which she and her partner were treated with a course of an antimicrobial. She is sexually active with one male partner, and they use condoms inconsistently. Her only medication is a combined oral contraceptive that she has been taking for the past 4 years. A Gram stain of her vaginal fluid is shown. Which of the following is the most likely causal organism?
A 35-year-old G2P0 presents to her physician to discuss the results of her 16-week obstetric screening tests. She has no complaints. Her previous pregnancy at 28 years of age was a spontaneous abortion in the first trimester. She has no history of gynecologic diseases. Her quadruple test shows the following findings: Alpha-fetoprotein Low Beta-hCG High Unconjugated estriol Low Inhibin A High Which of the following statements regarding the presented results is correct?
A 34-year-old woman, gravida 1, para 0, at 16 weeks' gestation comes to the physician for a routine prenatal visit. She feels well. She has no history of serious illness. She has smoked one pack of cigarettes daily for 10 years but quit when she learned she was pregnant. She does not drink alcohol or use illicit drugs. Her mother has type 1 diabetes mellitus, and her father has asthma. Current medications include a prenatal multivitamin. She appears well. Her vital signs are within normal limits. Physical examination shows no abnormalities. Serum studies show: Alpha-fetoprotein decreased Unconjugated estriol decreased Human chorionic gonadotropin increased Inhibin A increased During counseling regarding the potential for fetal abnormalities, the patient says that she would like a definitive diagnosis as quickly as possible. Which of the following is the most appropriate next step in management?
Practice by Chapter
First trimester screening
Practice Questions
Cell-free DNA screening
Practice Questions
Second trimester serum screening
Practice Questions
Ultrasound markers and anomaly screening
Practice Questions
Carrier screening for genetic disorders
Practice Questions
Cervical cancer screening in pregnancy
Practice Questions
Diabetes screening in pregnancy
Practice Questions
Gestational diabetes management
Practice Questions
Group B streptococcus screening
Practice Questions
Screening for preeclampsia risk factors
Practice Questions
Prenatal infection screening (TORCH, HIV, STIs)
Practice Questions
Genetic counseling principles
Practice Questions
Diagnostic testing (amniocentesis, CVS)
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app