
Screening tests — MCQs

On this page
A 17-year-old woman presents to the emergency department with dysuria. She denies any hematuria or dyspareunia. Her last menstrual period was 3 weeks ago, and she denies any recent sexual activity. Her temperature is 99.7°F (37.6°C), blood pressure is 127/67 mmHg, pulse is 90/min, and respirations are 17/min. An unusual odor is detected on inspection of the vagina and some gray discharge is noted. Speculum exam reveals a normal cervix and a bimanual exam is unremarkable for adnexal masses or tenderness. What is the next best step in management?
A 17-year-old girl comes to the physician because of left lower abdominal pain for 1 day. She describes the pain as 6 out of 10 in intensity. Over the past 5 months, she has had similar episodes of pain that occur once a month and last 1 to 2 days. Menses occur at regular 28-day intervals and last 5 to 6 days. Menarche was at the age of 13 years, and her last menstrual period was 2 weeks ago. She has been sexually active with 1 male partner in the past and has used condoms inconsistently. She tested negative for sexually transmitted infections on her last visit 6 months ago. Abdominal and pelvic examination shows no abnormalities. A urine pregnancy test is negative. Which of the following is the most appropriate next step in the management of this patient's symptoms?
A 17-year-old woman presents to the emergency department with abdominal and pelvic pain. She states it started 3 days ago and it has been getting gradually worse. She states it is diffuse and is located over her abdomen, pelvis, and inside her vagina. She also endorses vaginal pruritus and a discharge from her vagina. The patient works in an ice cream parlor and is sexually active with multiple different partners. Her temperature is 98.0°F (36.7°C), blood pressure is 122/80 mmHg, pulse is 82/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam is notable for a foul smelling vagina with a thin, white discharge. Her abdomen is diffusely tender. The patient is noted to be itching her vagina during the exam. Which of the following is the most appropriate initial step in management?
A 29-year-old nulligravid woman comes to the physician because of a 10-day history of small quantities of intermittent, blood-tinged discharge from her left nipple. There is no personal or family history of serious illness. She has smoked 1 pack of cigarettes daily for 5 years. Her last menstrual period was 12 days ago. She is sexually active and uses condoms inconsistently. Physical examination shows scant serosanguinous fluid expressible from the left nipple. There is no palpable breast mass or axillary lymphadenopathy. Examination shows no other abnormalities. Which of the following is the most appropriate next step in management?
A 30-year-old woman presents to the office with complaints of pain in her right breast for 5 days. The pain is moderate-to-intense and is localized to the upper quadrant of the right breast, and mainly to the areola for the past 48 hours. She adds that there is some nipple discharge on the same side and that the right breast is red. She was diagnosed with type 1 diabetes at the age of 10 years of age, for which she takes insulin. The family history is negative for breast and ovarian cancers, and endometrial disorders. She smokes one-half pack of cigarettes every day and binge drinks alcohol on the weekends. Two weeks ago she was hit by a volleyball while playing at the beach. There is no history of fractures or surgical procedures. The physical examination reveals a swollen, erythematous, and warm right breast with periareolar tenderness and nipple discharge. There are no palpable masses or lymphadenopathy. Which of the following is the most important risk factor for the development of this patient’s condition?
A 36-year-old G3P2002 presents to her obstetrician’s office for her first prenatal visit at ten weeks and two days gestation. She notes that she has felt nauseous the last several mornings and has been especially tired for a few weeks. Otherwise, she feels well. The patient has had two uncomplicated spontaneous vaginal deliveries at full term with her last child born six years ago. She is concerned about the risk of Down syndrome in this fetus, as her sister gave birth to an affected child at age 43. The patient has a history of generalized anxiety disorder, atopic dermatitis, and she is currently on escitalopram. At this visit, this patient’s temperature is 98.6°F (37.0°C), pulse is 70/min, blood pressure is 121/67 mmHg, and respirations are 13/min. The patient appears anxious, but overall comfortable, and cardiopulmonary and abdominal exams are unremarkable. Pelvic exam reveals normal female external genitalia, a closed and slightly soft cervix, a ten-week-sized uterus, and no adnexal masses. Which of the following is the best next step for definitively determining whether this patient’s fetus has Down syndrome?
A 29-year-old man presents to his primary care provider after complaining of a rash on his penis. He describes it as small painless growths that have developed over the past several months. They have slowly increased in size over time. His medical history is unremarkable. He has had several sexual partners and uses condoms inconsistently. He describes himself as having generally good health and takes no medication. On physical exam, his vital signs are normal. There are multiple cauliflower-like papular eruptions just under the glans penis. They are tan-pink and raised. Examination of the scrotum, perineum, and anus shows no abnormalities. There is no inguinal lymphadenopathy. The remainder of the physical exam shows no abnormalities. Which of the following is the most appropriate initial management?
A 27-year-old woman presents for her routine annual examination. She has no complaints. She has a 3-year-old child who was born via normal vaginal delivery with no complications. She had a Pap smear during her last pregnancy and the findings were normal. Her remaining past medical history is not significant, and her family history is also not significant. Recently, one of her close friends was diagnosed with breast cancer at the age of 36, and, after reading some online research, she wants to be checked for all types of cancer. Which of the following statements would be the best advice regarding the most appropriate screening tests for this patient?
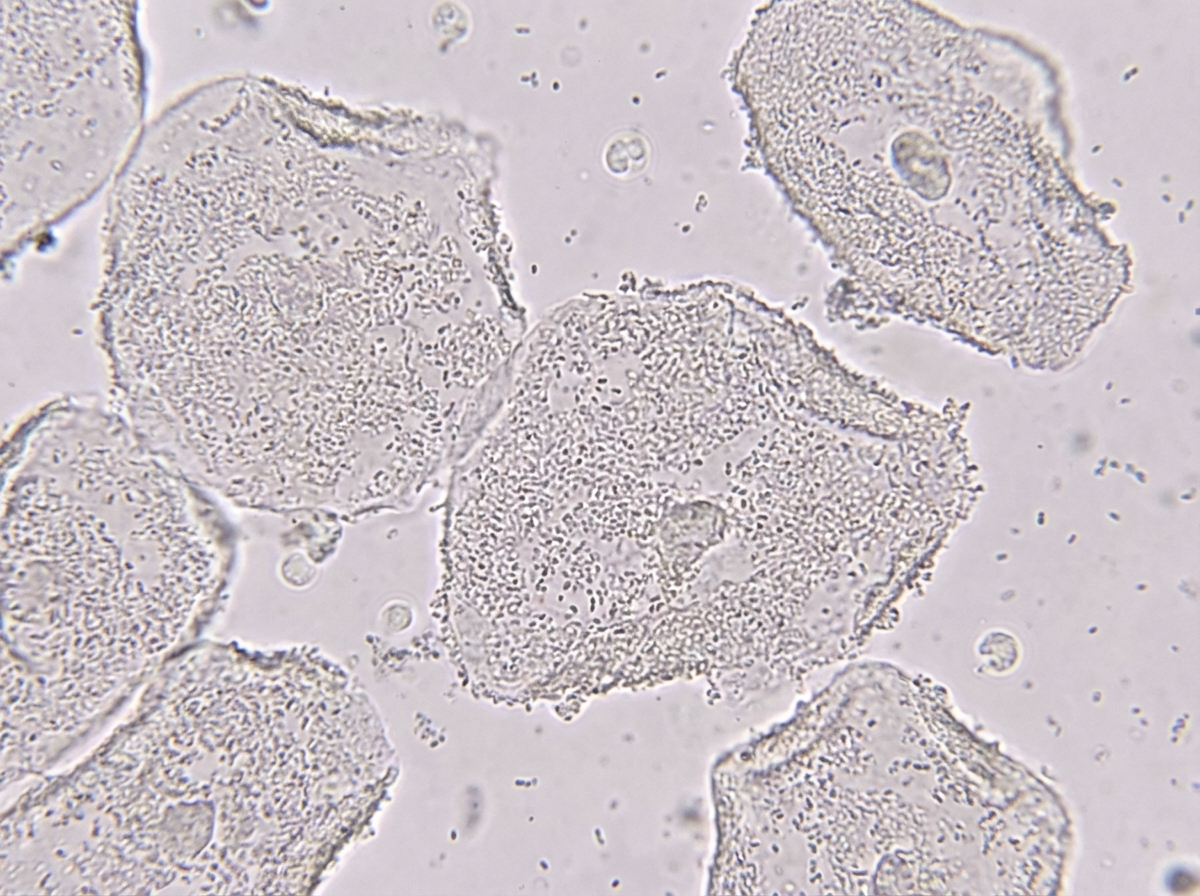
A previously healthy 23-year-old woman comes to the physician because of a 1-week history of vaginal discharge. She has no pain or pruritus. She is sexually active with one male partner and uses condoms inconsistently. Pelvic examination shows a malodorous gray vaginal discharge. Microscopic examination of the vaginal discharge is shown. Which of the following is the most likely diagnosis?
A 17-year-old high school student presents to the physician’s office for a health maintenance examination. He is a recent immigrant from Venezuela and has no complaints at this time. Past medical history is significant for appendicitis at age 10, treated with an appendectomy. He denies the use of alcohol and cigarettes. He admits to occasionally smoking marijuana with his friends. He is sexually active with 1 woman partner and uses condoms inconsistently. The vital signs are within normal limits. Physical examination is unremarkable except for a laparoscopic surgical scar on the right iliac region. Routine blood tests are pending. What is the most appropriate next step in management?
Practice by Chapter
First trimester screening
Practice Questions
Cell-free DNA screening
Practice Questions
Second trimester serum screening
Practice Questions
Ultrasound markers and anomaly screening
Practice Questions
Carrier screening for genetic disorders
Practice Questions
Cervical cancer screening in pregnancy
Practice Questions
Diabetes screening in pregnancy
Practice Questions
Gestational diabetes management
Practice Questions
Group B streptococcus screening
Practice Questions
Screening for preeclampsia risk factors
Practice Questions
Prenatal infection screening (TORCH, HIV, STIs)
Practice Questions
Genetic counseling principles
Practice Questions
Diagnostic testing (amniocentesis, CVS)
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app