
Prenatal Care — MCQs

On this page
An otherwise healthy 15-year-old girl is brought to the physician for evaluation of severe acne that involves her face, chest, and back. It has not improved with her current combination therapy of oral cephalexin and topical benzoyl peroxide. She is sexually active with one male partner, and they use condoms consistently. Facial scarring and numerous comedones are present, with sebaceous skin lesions on her face, chest, and back. Which of the following is indicated prior to initiating the appropriate treatment in this patient?
A 33-year-old pregnant woman in the 28th week of gestation presents to the emergency department for evaluation of bilateral edema of her legs. It seems to worsen at the end of the day and has lasted for the past 3 weeks. History reveals that this is her 3rd pregnancy. Vital signs include: blood pressure 120/80 mm Hg, heart rate 74/min, respiratory rate 18/min, and temperature 36.6°C (98.0°F). Body mass index is 36 kg/m2. Physical examination reveals bilateral leg edema with engorged surface veins. A photograph of the patient’s legs is shown. Which of the following is the best initial management of the patient?
A 22-year-old G1P1 woman comes to the clinic asking about “the morning after pill.” She reports that she had sexual intercourse with her boyfriend last night and she thinks the condom broke. She is not using any other form of contraception. She reports her last menstrual period was 10 days ago, and they are normally regular. The patient’s medical history is significant for obesity, asthma and allergic rhinitis. Her medications include albuterol and occasional intranasal corticosteroids. She has no history of sexually transmitted diseases and is sexually active with only her current boyfriend of 5 years. The patient denies genitourinary symptoms. Her temperature is 98°F (36.7°C), blood pressure is 112/74 mmHg, pulse is 63/min, and respirations are 12/min with an oxygen saturation of 99% O2 on room air. Physical examination, including a pelvic exam, shows no abnormalities. The patient is worried because she is back in graduate school and cannot afford another child. Which of the following is the most effective emergency contraception?
A 37-year-old woman, gravida 3, para 3, comes to the physician for a follow-up examination. She gave birth to her third child 8 months ago and now wishes to start a contraception method. Prior to her most recent pregnancy, she used a combined estrogen-progestin pill. Which of the following aspects of her history would be a contraindication for restarting an oral contraceptive pill?
A 22-year-old woman comes to the physician because of a 1-week history of nausea and vomiting. She has not had fever, abdominal pain, diarrhea, or vaginal bleeding. She does not remember the date of her last menstrual period. She uses oral contraceptive pills but occasionally forgot to take them. She had pelvic inflammatory disease 2 years ago and was treated with antibiotics. Her temperature is 37°C (98.6°F), pulse is 110/min, respirations are 16/min, and blood pressure is 118/75 mm Hg. Physical examination shows no abnormalities. Pelvic examination shows a normal appearing vagina, cervix, uterus, and adnexa. A urine pregnancy test is positive. Her serum β-human chorionic gonadotropin concentration is 805 mIU/mL. Which of the following is the most appropriate next step in diagnosis?
A healthy 31-year-old woman comes to the physician because she is trying to conceive. She is currently timing the frequency of intercourse with at-home ovulation test kits. An increase in the levels of which of the following is the best indicator that ovulation has occurred?
A 17-year-old girl comes to your outpatient clinic. She is sexually active with multiple partners and requests a prescription for oral contraceptive pills. A urine pregnancy test in your office is negative. Which of the following is the most appropriate next step?
A 28-year-old woman, gravida 1, para 0, at 10 weeks' gestation comes to the physician for her initial prenatal visit. She has no history of serious illness, but reports that she is allergic to penicillin. Vital signs are within normal limits. The lungs are clear to auscultation, and cardiac examination shows no abnormalities. Transvaginal ultrasonography shows an intrauterine pregnancy with no abnormalities. The fetal heart rate is 174/min. Routine prenatal laboratory tests are drawn. Rapid plasma reagin (RPR) test is 1:128 and fluorescent treponemal antibody absorption test (FTA-ABS) is positive. Which of the following is the most appropriate next step in management?
A 24-year-old G1P0000 presents for her first obstetric visit and is found to be at approximately 8 weeks gestation. She has no complaints aside from increased fatigue and occasional nausea. The patient is a recent immigrant from Africa and is currently working as a babysitter for several neighborhood children. One of them recently had the flu, and another is home sick with chickenpox. The patient has no immunization records and does not recall if she has had any vaccinations. She is sexually active with only her husband, has never had a sexually transmitted disease, and denies intravenous drug use. Her husband has no past medical history. Exam at this visit is unremarkable. Her temperature is 98.7°F (37.1°C), blood pressure is 122/76 mmHg, pulse is 66/min, and respirations are 12/min. Which of the following immunizations should this patient receive at this time?
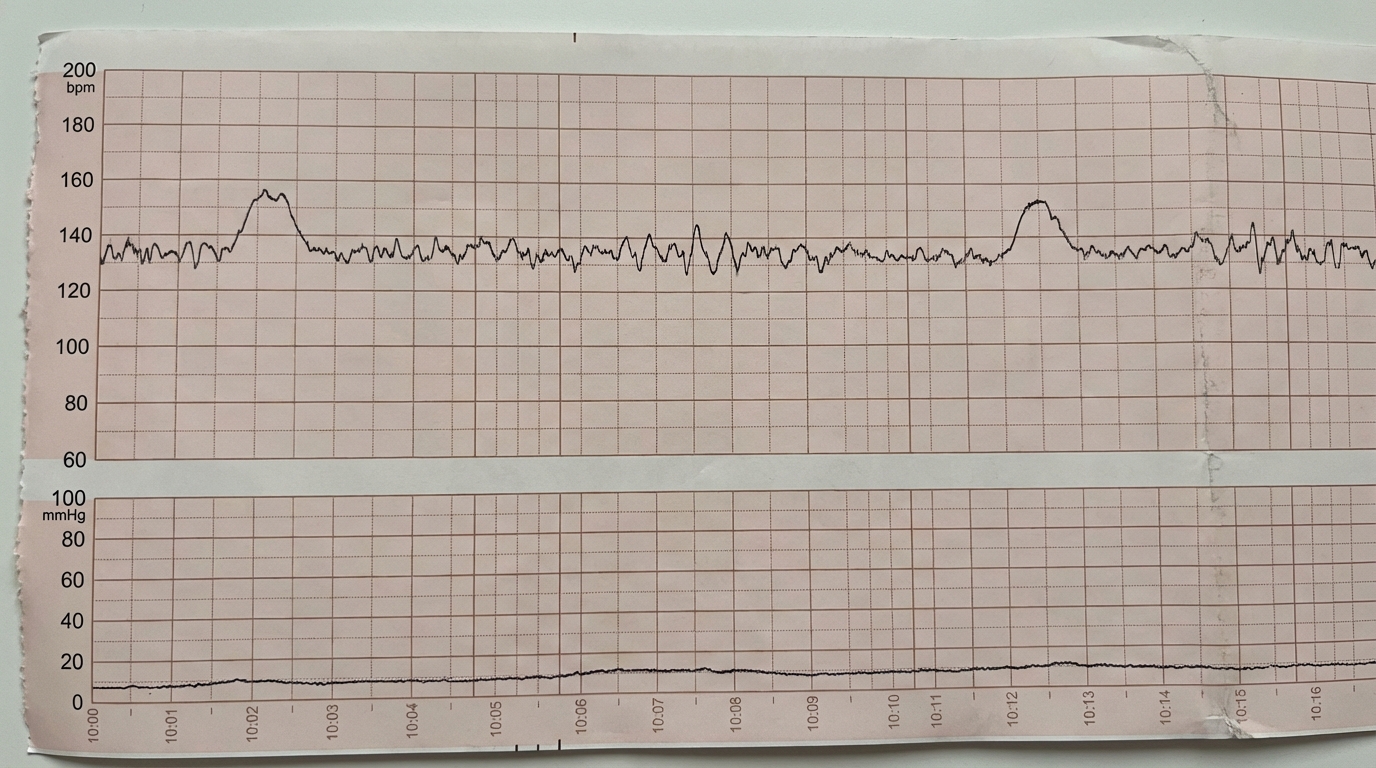
A 27-year-old woman, gravida 2, para 1, at 32 weeks' gestation comes to the physician for a prenatal visit. She feels that her baby's movements have decreased recently. She says that she used to feel 10–12 movements/hour earlier, but that it has recently decreased to about 7–8/hour. Pregnancy and delivery of her first child were uncomplicated. Medications include folic acid and a multivitamin. Her temperature is 37.2°C (99°F), and blood pressure is 108/60 mm Hg. Pelvic examination shows a uterus consistent in size with a 32-week gestation. The fetus is in a transverse lie presentation. The fetal heart rate is 134/min. A 14-minute recording of the nonstress test is shown. Which of the following is the most appropriate next step in managing this patient?
Practice by Chapter
Routine prenatal visit schedule
Practice Questions
Nutrition in pregnancy
Practice Questions
Weight gain recommendations
Practice Questions
Exercise in pregnancy
Practice Questions
Medication safety in pregnancy
Practice Questions
Immunizations in pregnancy
Practice Questions
Management of common pregnancy complaints
Practice Questions
Fetal growth assessment
Practice Questions
Fetal movement monitoring
Practice Questions
Antepartum fetal surveillance (NST, BPP)
Practice Questions
Anemia in pregnancy
Practice Questions
Travel during pregnancy
Practice Questions
Patient education topics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app