
Fetal movement monitoring — MCQs

You have been entrusted with the task of finding the causes of low birth weight in infants born in the health jurisdiction for which you are responsible. In 2017, there were 1,500 live births and, upon further inspection of the birth certificates, 108 of these children had a low birth weight (i.e. lower than 2,500 g), while 237 had mothers who smoked continuously during pregnancy. Further calculations have shown that the risk of low birth weight in smokers was 14% and in non-smokers, it was 7%, while the relative risk of low birth weight linked to cigarette smoking during pregnancy was 2%. In other words, women who smoked during pregnancy were twice as likely as those who did not smoke to deliver a low-weight infant. Using this data, you are also asked to calculate how much of the excess risk for low birth weight, in percentage terms, can be attributed to smoking. What is the attributable risk percentage for smoking leading to low birth weight?
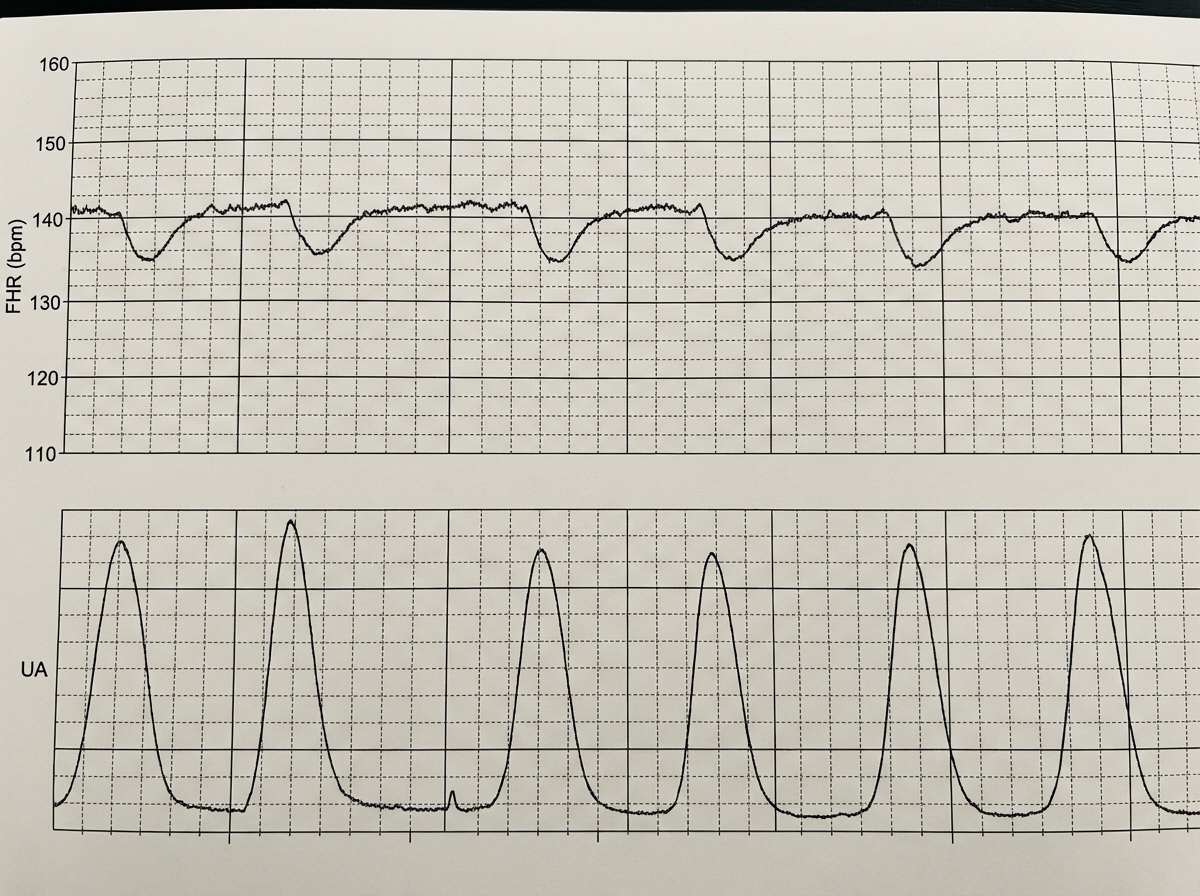
A 39-year-old woman, gravida 5, para 4, at 41 weeks' gestation is brought to the hospital because of regular uterine contractions that started 2 hours ago. Pregnancy has been complicated by iron deficiency anemia treated with iron supplements. Pelvic examination shows the cervix is 90% effaced and 7-cm dilated; the vertex is at -1 station. Fetal heart tracing is shown. The patient is repositioned, O2 therapy is initiated, and amnioinfusion is done. A repeat assessment after 20 minutes shows a similar cervical status, and no changes in the fetal heart tracing, and less than 5 contractions in a period of 10 minutes.What is the most appropriate next step in management?
A 42-year-old G1P0 woman presents to an obstetrician for her first prenatal visit. She has been pregnant for about 10 weeks and is concerned about how pregnancy will affect her health. Specifically, she is afraid that her complicated medical history will be adversely affected by her pregnancy. Her past medical history is significant for mild polycythemia, obesity hypoventilation syndrome, easy bleeding, multiple sclerosis, and aortic regurgitation. Which of these disorders is most likely to increase in severity during the course of the pregnancy?
A 27-year old primigravid woman at 37 weeks' gestation comes to the emergency department because of frequent contractions for 4 hours. Her pregnancy has been complicated by hyperemesis gravidarum which subsided in the second trimester. The contractions occur every 10–15 minutes and have been increasing in intensity and duration since onset. Her temperature is 37.1°C (98.8°F), pulse is 110/min, and blood pressure is 140/85 mm Hg. Uterine contractions are felt on palpation. Pelvic examination shows clear fluid in the vagina. The cervix is 50% effaced and 3 cm dilated. After 4 hours the cervix is 80% effaced and 6 cm dilated. Pelvic examination is inconclusive for the position of the fetal head. The fetal heart rate is reassuring. Which of the following is the most appropriate next step?
A 15-month-old boy is brought to the pediatrician’s office by his mother due to abnormal muscle tone and an inability to walk. He was able to control his head at 5 months of age, roll at 8 months of age, sit at 11 months of age, and develop hand preference at 13 months of age. On physical exam, he is observed to asymmetrically crawl. He has a velocity-dependent increase in tone and 3+ biceps and patellar reflexes. His startle, asymmetric tonic neck, and Babinski reflexes are present. Which of the following is the most common risk factor for developing this patient’s clinical presentation?
A 24-year-old primigravida at 28 weeks gestation presents to the office stating that she “can’t feel her baby kicking anymore.” She also noticed mild-to-moderate vaginal bleeding. A prenatal visit a few days ago confirmed the fetal cardiac activity by Doppler. The medical history is significant for GERD, hypertension, and SLE. The temperature is 36.78°C (98.2°F), the blood pressure is 125/80 mm Hg, the pulse is 70/min, and the respiratory rate is 14/min. Which of the following is the next best step in evaluation?
A 26-year-old G1P0 female who is 39 weeks pregnant presents to the emergency department in labor. She reports following her primary care physician’s recommendations throughout her pregnancy and has not had any complications. During delivery, the baby’s head turtled back into the vaginal canal and did not advance any further. The neonatal intensivist was called for shoulder dystocia and a baby girl was able to be delivered vaginally 6 minutes later. Upon initial assessment, the baby appeared pale throughout, had her arms and legs flexed without active motion, and had some flexion of extremities when stimulated. Her pulse is 120/min and had irregular respirations. What is this baby’s initial APGAR score?
A 30-year-old woman, gravida 2, para 1, at 38 weeks' gestation comes to the hospital for regular, painful contractions that have been increasing in frequency. Her pregnancy has been complicated by gestational diabetes treated with insulin. Pelvic examination shows the cervix is 50% effaced and 4 cm dilated; the vertex is at -1 station. Ultrasonography shows no abnormalities. A tocometer and Doppler fetal heart monitor are placed on the patient's abdomen. The fetal heart rate monitoring strip shows a baseline heart rate of 145/min with a variability of ≥ 15/min. Within a 20-minute recording, there are 7 uterine contractions, 4 accelerations, and 3 decelerations that have a nadir occurring within half a minute. The decelerations occur at differing intervals relative to the contractions. Which of the following is the most appropriate next step in the management of this patient?
A 9-month-old boy is brought to the physician because of abnormal crawling and inability to sit without support. A 2nd-trimester urinary tract infection that required antibiotic use and a spontaneous preterm birth via vaginal delivery at 36 weeks’ gestation both complicated the mother’s pregnancy. Physical examination shows a scissoring posture of the legs when the child is suspended by the axillae. Examination of the lower extremities shows brisk tendon reflexes, ankle clonus, and upward plantar reflexes bilaterally. When encouraged by his mother, the infant crawls forward by using normal reciprocal movements of his arms, while his legs drag behind. A brain MRI shows scarring and atrophy in the white matter around the ventricles with ventricular enlargement. Which of the following is most likely associated with the findings in this child?
A 30-year-old primigravida schedules an appointment with her obstetrician for a regular check-up. She says that everything is fine, although she reports that her baby has stopped moving as much as previously. She is 22 weeks gestation. She denies any pain or vaginal bleeding. The obstetrician performs an ultrasound and also orders routine blood and urine tests. On ultrasound, there is no fetal cardiac activity or movement. The patient is asked to wait for 1 hour, after which the scan is to be repeated. The second scan shows the same findings. Which of the following is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app