
Prenatal Care — MCQs

On this page
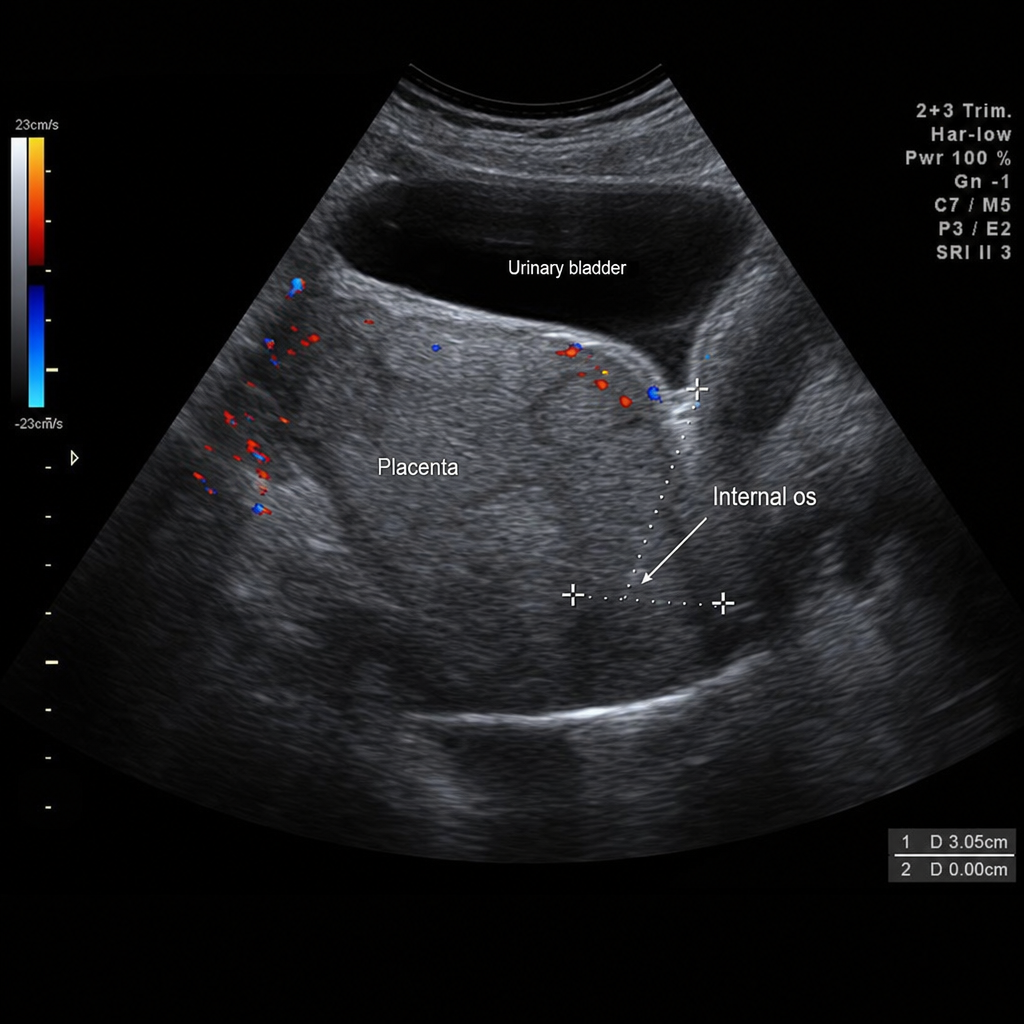
A 25-year-old woman, G1P0, at 30 weeks of gestation is brought to the emergency department with sudden-onset painless bright red vaginal bleeding. She reports two prior episodes of spotting over the past 3 weeks. Vital signs: BP 110/70 mmHg, HR 98 bpm, RR 16/min. Fetal heart rate tracing shows a baseline of 145 bpm with moderate variability and no decelerations. Transabdominal ultrasound shows placenta completely covering the internal os. Which of the following is the most appropriate immediate management?

A 25-year-old G1P0 woman at 32 weeks of gestation presents with sudden-onset painless vaginal bleeding. She reports soaking two pads in the past hour. She denies contractions, leaking fluid, or trauma. Vital signs: BP 110/70 mmHg, HR 102 bpm, RR 18/min, SpO₂ 99%. Fetal heart rate tracing is Category I. Transabdominal ultrasound of the lower uterine segment demonstrates complete placenta previa, with the placenta completely covering the internal cervical os. Based on the ultrasound findings, which of the following is the most appropriate immediate management?
A 34-year-old woman presents at 6 weeks of delivery. She wants contraception for the next 3 years. What will be the best contraceptive method in this case?
A GSP4 woman comes for routine sonography for the first time. She has four daughters and expresses a desire for a boy this time, asking for sex determination. To abide by ethical guidelines, what should you do?
What is the typical time between fertilization and implantation?
Practice by Chapter
Routine prenatal visit schedule
Practice Questions
Nutrition in pregnancy
Practice Questions
Weight gain recommendations
Practice Questions
Exercise in pregnancy
Practice Questions
Medication safety in pregnancy
Practice Questions
Immunizations in pregnancy
Practice Questions
Management of common pregnancy complaints
Practice Questions
Fetal growth assessment
Practice Questions
Fetal movement monitoring
Practice Questions
Antepartum fetal surveillance (NST, BPP)
Practice Questions
Anemia in pregnancy
Practice Questions
Travel during pregnancy
Practice Questions
Patient education topics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app