
Balloon tamponade techniques — MCQs

A 24-year-old primigravida presents at 36 weeks gestation with vaginal bleeding, mild abdominal pain, and uterine contractions that appeared after bumping into a handrail. The vital signs are as follows: blood pressure 130/80 mm Hg, heart rate 79/min, respiratory rate 12/min, and temperature 36.5℃ (97.7℉). The fetal heart rate was 145/min. Uterine fundus is at the level of the xiphoid process. Slight uterine tenderness and contractions are noted on palpation. The perineum is bloody. The gynecologic examination shows no vaginal or cervical lesions. The cervix is long and closed. Streaks of bright red blood are passing through the cervix. A transabdominal ultrasound shows the placenta to be attached to the lateral uterine wall with a marginal retroplacental hematoma (an approximate volume of 150 ml). The maternal hematocrit is 36%. What is the next best step in the management of this patient?
A 30-year-old woman, gravida 2, para 1, at 42 weeks' gestation is admitted to the hospital in active labor. Pregnancy has been complicated by gestational diabetes, for which she has been receiving insulin injections. Her first child was delivered by lower segment transverse cesarean section because of a nonreassuring fetal heart rate. Her pulse is 90/min, respirations are 18/min, and blood pressure is 135/80 mm Hg. The fetal heart rate tracing shows a baseline heart rate of 145/min and moderate variation with frequent accelerations and occasional early decelerations. She undergoes an elective repeat lower segment transverse cesarean section with complete removal of the placenta. Shortly after the operation, she starts having heavy uterine bleeding with passage of clots. Examination shows a soft uterus on palpation. Her bleeding continues despite fundal massage and the use of packing, oxytocin, misoprostol, and carboprost. Her pulse rate is now 120/min, respirations are 20/min, and blood pressure is 90/70 mm Hg. Her hemoglobin is 8 g/dL, hematocrit is 24%, platelet count is 120,000 mm3, prothrombin time is 11 seconds, and partial thromboplastin time is 30 seconds. Mass transfusion protocol is activated and a B-Lynch uterine compression suture is placed to control her bleeding. Which of the following is the mostly likely cause of her postpartum complication?
Five minutes after initiating a change of position and oxygen inhalation, the oxytocin infusion is discontinued. A repeat CTG that is done 10 minutes later shows recurrent variable decelerations and a total of 3 uterine contractions in 10 minutes. Which of the following is the most appropriate next step in management?
Thirty minutes after vaginal delivery of a 2780-g (6-lb 2-oz) newborn at term, a 25-year-old woman, gravida 1, para 1, has heavy vaginal bleeding. Her pregnancy was complicated by pre-eclampsia. Her pulse is 111/min and blood pressure is 95/65 mm Hg. Physical examination shows a fundal height 2 inches below the xiphoid process of the sternum. A drug with which of the following mechanisms of action is most appropriate for this patient?
Thirty minutes after normal vaginal delivery of twins, a 35-year-old woman, gravida 5, para 4, has heavy vaginal bleeding with clots. Physical examination shows a soft, enlarged, and boggy uterus. Despite bimanual uterine massage, administration of uterotonic drugs, and placement of an intrauterine balloon for tamponade, the bleeding continues. A hysterectomy is performed. Vessels running through which of the following structures must be ligated during the surgery to achieve hemostasis?
A 57-year-old man is brought to the emergency department by his family because of several episodes of vomiting of blood in the past 24 hours. He has a history of alcoholic cirrhosis and is being treated for ascites with diuretics and for encephalopathy with lactulose. His vital signs include a temperature of 36.9°C (98.4°F), pulse of 85/min, and blood pressure of 80/52 mm Hg. On examination, he is confused and unable to give a complete history. He is noted to have jaundice, splenomegaly, and multiple spider angiomas over his chest. Which of the following is the best initial management of this patient?
A 29-year-old G1P0 presents to her obstetrician for her first prenatal care visit at 12 weeks gestation by last menstrual period. She states that her breasts are very tender and swollen, and her exercise endurance has declined. She otherwise feels well. She is concerned about preterm birth, as she heard that certain cervical procedures increase the risk. The patient has a gynecologic history of loop electrosurgical excision procedure (LEEP) for cervical dysplasia several years ago and has had negative Pap smears since then. She also has mild intermittent asthma that is well controlled with occasional use of her albuterol inhaler. At this visit, this patient’s temperature is 98.6°F (37.0°C), pulse is 69/min, blood pressure is 119/61 mmHg, and respirations are 13/min. Cardiopulmonary exam is unremarkable, and the uterine fundus is just palpable at the pelvic brim. Pelvic exam reveals normal female external genitalia, a closed and slightly soft cervix, a 12-week-size uterus, and no adnexal masses. Which of the following is the best method for evaluating for possible cervical incompetence in this patient?
A 27-year-old woman, gravida 2, para 1, at 36 weeks' gestation comes to the physician for a prenatal visit. She feels well. Fetal movements are adequate. This is her 7th prenatal visit. She had an ultrasound scan performed 1 month ago that showed a live intrauterine pregnancy consistent with a 32-week gestation with no anomalies. She had a Pap smear performed 1 year ago, which was normal. Vital signs are within normal limits. Pelvic examination shows a uterus consistent in size with a 36-week gestation. Her blood group and type is A negative. Which of the following is the most appropriate next step in management?
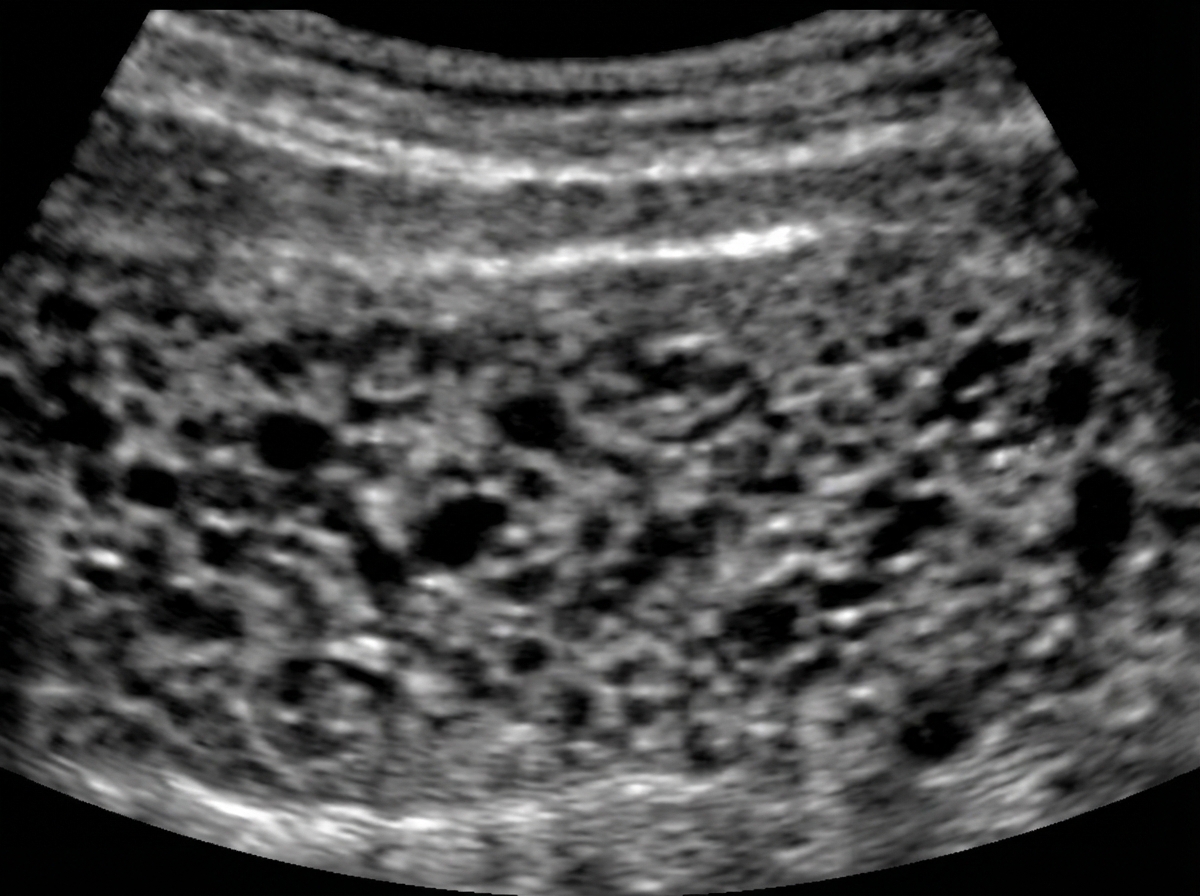
A 30-year-old woman comes to the primary care physician because she has felt nauseous and fatigued for 3 weeks. Menses occur at irregular 24- to 33-day intervals and last for 4–6 days. Her last menstrual period was 7 weeks ago. Her temperature is 37°C (98.6°F), pulse is 95/min, and blood pressure is 100/70 mm Hg. Pelvic examination shows an enlarged uterus. Her serum β-hCG concentration is 96,000 mIU/mL (N < 5). An abdominal ultrasound is shown. Which of the following is the most likely diagnosis?
29-year-old G2P2002 presents with foul-smelling lochia and fever. She is post-partum day three status-post cesarean section due to eclampsia. Her temperature is 101 F, and heart rate is 103. She denies chills. On physical exam, lower abdominal and uterine tenderness is present. Leukocytosis with left shift is seen in labs. Which of the following is the next best step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app