
Postpartum hemorrhage — MCQs

On this page
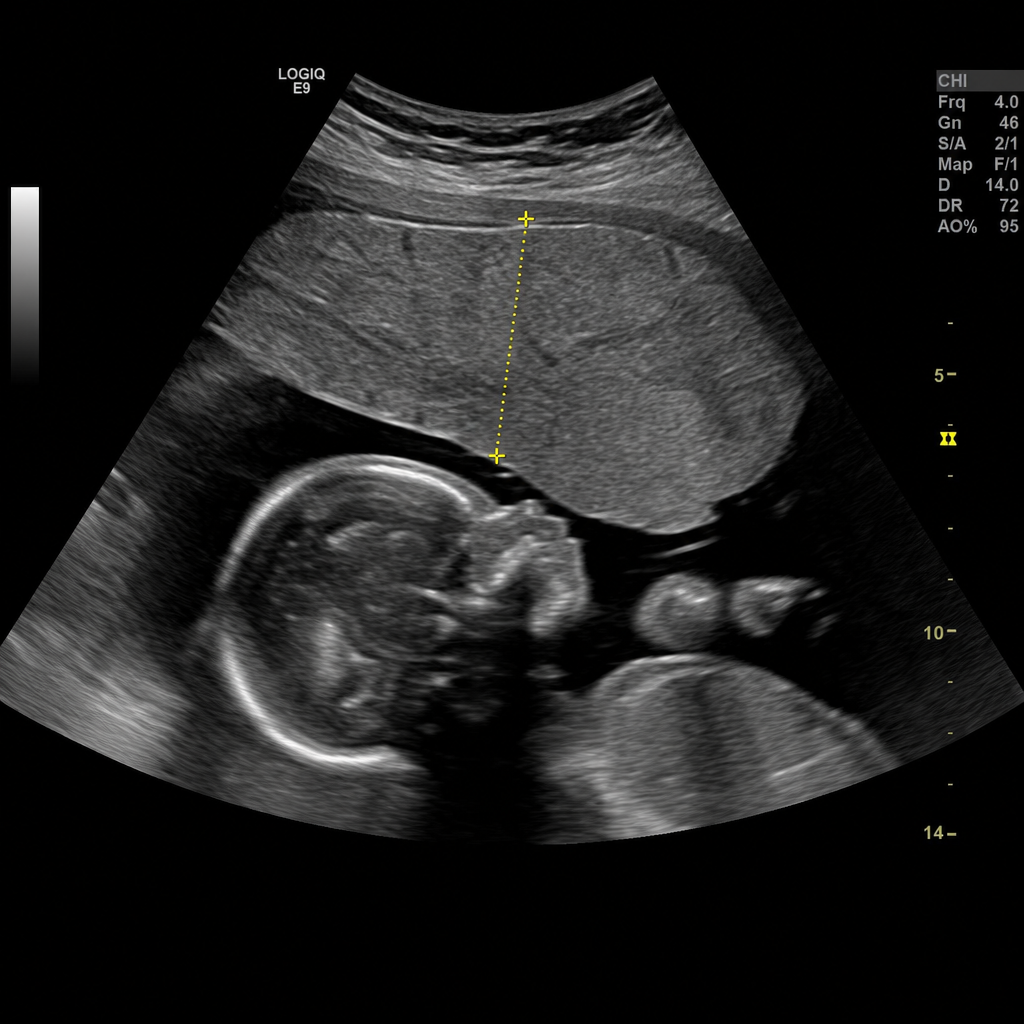
A 34-year-old woman, G2P1, at 32 weeks of gestation presents with sudden-onset painless bright red vaginal bleeding. She soaked two pads in the past hour. She denies contractions or trauma. Her prior delivery was by cesarean section for breech presentation. Vital signs: BP 110/70 mmHg, HR 96 bpm, temperature 36.8°C. Fetal heart rate tracing shows a baseline of 150 bpm with moderate variability and no decelerations. Transabdominal ultrasound demonstrates an anterior placenta completely overlying the internal cervical os. Based on the imaging findings and clinical context, which of the following is the most appropriate immediate management?
A pregnant woman with a known case of asthma is experiencing postpartum hemorrhage (PPH). Which drug is contraindicated?
A 27-year-old woman who delivered a female child 9 months ago presents with complaints of absent periods since childbirth. She has been using contraceptive methods for family planning. Her serum beta-hCG level is 4.9 mIU/ ml , prolactin level is $88 \mathrm{ng} / \mathrm{ml}$, and TSH is 3.8 $\mu \mathrm{IU} / \mathrm{ml}$. What is the most likely reason for her amenorrhea?
The patient declines the use of oxytocin or any other further testing and decides to await a spontaneous delivery. Five weeks later, she comes to the emergency department complaining of vaginal bleeding for 1 hour. Her pulse is 110/min, respirations are 18/min, and blood pressure is 112/76 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 97%. Pelvic examination shows active vaginal bleeding. Laboratory studies show: Hemoglobin 12.8 g/dL Leukocyte count 10,300/mm3 Platelet count 105,000/mm3 Prothrombin time 26 seconds (INR=1.8) Serum Na+ 139 mEq/L K+ 4.1 mEq/L Cl- 101 mEq/L Urea nitrogen 42 mg/dL Creatinine 2.8 mg/dL Which of the following is the most likely underlying mechanism of this patient's symptoms?
Forty-five minutes after the spontaneous delivery of a male newborn at 39 weeks' gestation, a 27-year-old primigravid woman complains of worsening abdominal pain and dizziness. The patient was admitted to the hospital 5 hours prior because of spontaneous rupture of membranes. During labor, she experienced a brief episode of inadequate contractions which resolved following administration of IV oxytocin. The placenta was extracted manually after multiple attempts of controlled cord traction and fundal pressure. The patient has no history of serious illness except for occasional nosebleeds. The pregnancy was uncomplicated. Her pulse is 110/min and blood pressure is 85/50 mmHg. There is brisk vaginal bleeding from a round mass protruding from the vagina. The fundus is not palpable on abdominal exam. Which of the following is the most likely cause of bleeding in this patient?
A 62-year-old woman presents to the primary care physician with complaints of urinary leakage over the last 2 months. History reveals that the leakage occurred when she sneezed, laughed, or coughed. Her menopause occurred 11 years ago and she is a mother of 3 children. Vital signs include blood pressure 120/80 mm Hg, heart rate 84/min, respiratory rate 18/min, and temperature 36.6°C (98.0°F). Physical examination is unremarkable. Urinalysis reveals: Color Yellow Clarity/turbidity Clear pH 5.5 Specific gravity 1.015 Nitrites Negative Leukocyte esterase Negative Which of the following is the best initial management for this patient?
A 24-year-old woman presents to her primary care physician for breast pain. She states that recently she has experienced bilateral breast fullness and tenderness. She also feels that her breasts feel warm. She gave birth to an infant girl at 40 weeks gestation 2 weeks ago. She reports that her baby has been doing well and that she has been feeding her on formula only successfully. Physical exam is notable for bilateral breast fullness with tenderness upon palpation. The patient's breasts feel warmer than her forehead. Which of the following is the best next step in management?
Six hours after giving birth to a healthy 3100 g (6 lb 13oz) girl, a 40-year-old woman, gravida 1, para 1 suddenly has a tonic-clonic seizure for 2-minutes while on the ward. She had been complaining of headache, blurry vision, and abdominal pain for an hour before the incident. Her pregnancy was complicated by gestational hypertension and iron deficiency anemia. Her medications until birth included labetalol, iron supplements, and a multivitamin. Her temperature is 37°C (98.7°F), pulse is 95/min, respirations are 18/min, and blood pressure is 152/100 mm Hg. The cranial nerves are intact. Muscle strength is normal. Deep tendon reflexes are 3+ with a shortened relaxation phase. Which of the following is the most appropriate next step in management?
A 35-year-old woman comes to the physician because of swelling of her right breast for the past 4 days. She also reports malaise and some pain with breastfeeding. Three weeks ago, she delivered a healthy 3500-g (7.7-lb) girl. She has no history of serious illness. Her mother died of breast cancer at the age of 55 years. Her only medication is a multivitamin. Her temperature is 38°C (100.4°F). Examination shows a tender, firm, swollen, erythematous right breast. Examination of the left breast shows no abnormalities. Which of the following is the most appropriate next step in management?
Thirty minutes after normal vaginal delivery of twins, a 35-year-old woman, gravida 5, para 4, has heavy vaginal bleeding with clots. Physical examination shows a soft, enlarged, and boggy uterus. Despite bimanual uterine massage, administration of uterotonic drugs, and placement of an intrauterine balloon for tamponade, the bleeding continues. A hysterectomy is performed. Vessels running through which of the following structures must be ligated during the surgery to achieve hemostasis?
Practice by Chapter
Definition and classification
Practice Questions
Risk factors for postpartum hemorrhage
Practice Questions
Uterine atony management
Practice Questions
Retained placenta management
Practice Questions
Genital tract trauma repair
Practice Questions
Coagulation disorders in obstetrics
Practice Questions
Medical management of PPH
Practice Questions
Surgical management of PPH
Practice Questions
Balloon tamponade techniques
Practice Questions
Uterine compression sutures
Practice Questions
Postpartum hemorrhage protocols
Practice Questions
Blood product replacement strategies
Practice Questions
Prevention of postpartum hemorrhage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app