
Labor Complications — MCQs

On this page
A 29-year-old G2P1 at 35 weeks gestation presents to the obstetric emergency room with vaginal bleeding and severe lower back pain. She reports the acute onset of these symptoms 1 hour ago while she was outside playing with her 4-year-old son. Her prior birthing history is notable for an emergency cesarean section during her first pregnancy. She received appropriate prenatal care during both pregnancies. She has a history of myomectomy for uterine fibroids. Her past medical history is notable for diabetes mellitus. She takes metformin. Her temperature is 99.0°F (37.2°C), blood pressure is 104/68 mmHg, pulse is 120/min, and respirations are 20/min. On physical examination, the patient is in moderate distress. Large blood clots are removed from the vaginal vault. Contractions are occurring every 2 minutes. Delayed decelerations are noted on fetal heart monitoring. Which of the following is the most likely cause of this patient's symptoms?
A 37-year-old G2P1 woman presents to the clinic complaining of amenorrhea. She reports that she has not had a period for 2 months. A urine pregnancy test that she performed yesterday was negative. She is sexually active with her husband and uses regular contraception. Her past medical history is significant for diabetes and a dilation and curettage procedure 4 months ago for an unviable pregnancy. She denies any discharge, abnormal odor, abnormal bleeding, dysmenorrhea, or pain but endorses a 10-pound intentional weight loss over the past 3 months. A pelvic examination is unremarkable. What is the most likely explanation for this patient’s presentation?
A 32-year-old woman visits her family physician for a routine health check-up. During the consult, she complains about recent-onset constipation, painful defecation, and occasional pain with micturition for the past few months. Her menstrual cycles have always been regular with moderate pelvic pain during menses, which is relieved with pain medication. However, in the last 6 months, she has noticed that her menses are “heavier” with severe lower abdominal cramps that linger for 4–5 days after the last day of menstruation. She and her husband are trying to conceive a second child, but lately, she has been unable to have sexual intercourse due to pain during sexual intercourse. During the physical examination, she has tenderness in the lower abdomen with no palpable mass. Pelvic examination reveals a left-deviated tender cervix, a tender retroverted uterus, and a left adnexal mass. During the rectovaginal examination, nodules are noted. What is the most likely diagnosis for this patient?
A 30-year-old woman, gravida 2, para 1, at 31 weeks' gestation is admitted to the hospital because her water broke one hour ago. Pregnancy has been complicated by iron deficiency anemia and hypothyroidism treated with iron supplements and L-thyroxine, respectively. The patient followed-up with her gynecologist on a regular basis throughout the pregnancy. Pregnancy and delivery of her first child were uncomplicated. Pulse is 90/min, respirations are 17/min, and blood pressure is 130/80 mm Hg. The abdomen is nontender. She has had 8 contractions within the last hour. Pelvic examination shows cervical dilation of 3 cm. The fetal heart rate is 140/min with no decelerations. In addition to administration of dexamethasone and terbutaline, which of the following is the most appropriate next step in the management of this patient?
A 39-year-old woman, gravida 4, para 4, comes to the physician because of a 5-month history of painful, heavy menses. Menses previously occurred at regular 28-day intervals and lasted 3 days with normal flow. They now last 7–8 days and the flow is heavy with the passage of clots. Pelvic examination shows a tender, uniformly enlarged, flaccid uterus consistent in size with an 8-week gestation. A urine pregnancy test is negative. Which of the following is the most likely cause of this patient's findings?
A 46-year-old woman presents to the clinic complaining that she “wets herself.” She states that over the past year she has noticed increased urinary leakage. At first it occurred only during her job, which involves restocking shelves with heavy appliances. Now she reports that she has to wear pads daily because leakage of urine will occur with simply coughing or sneezing. She denies fever, chills, dysuria, hematuria, or flank pain. She has no significant medical or surgical history, and takes no medications. Her last menstrual period was 8 months ago. She has 3 healthy daughters that were born by vaginal delivery. Which of the following tests, if performed, would most likely identify the patient’s diagnosis?
A 68-year-old woman comes to the physician for the evaluation of loss of urine for the last year. The patient states that she loses control over her bladder when walking or standing up. She reports frequent, small-volume urine losses with no urge to urinate prior to the leakage. She tried to strengthen her pelvic muscles with supervised Kegel exercises and using a continence pessary but her symptoms did not improve. The patient is sexually active with her husband. She has type 2 diabetes mellitus controlled with metformin. She does not smoke or drink alcohol. Vital signs are within normal limits. Her hemoglobin A1c is 6.3% and fingerstick blood glucose concentration is 110 mg/dL. Which of the following is the most appropriate next step in the management of this patient?
A 37-year-old woman presents with an inability to void in the hours after giving birth to her first child via vaginal delivery. Her delivery involved the use of epidural anesthesia as well as pelvic trauma from the use of forceps. She is currently experiencing urinary leakage and complains of increased lower abdominal pressure. Which of the following is the most appropriate treatment for this patient’s condition?
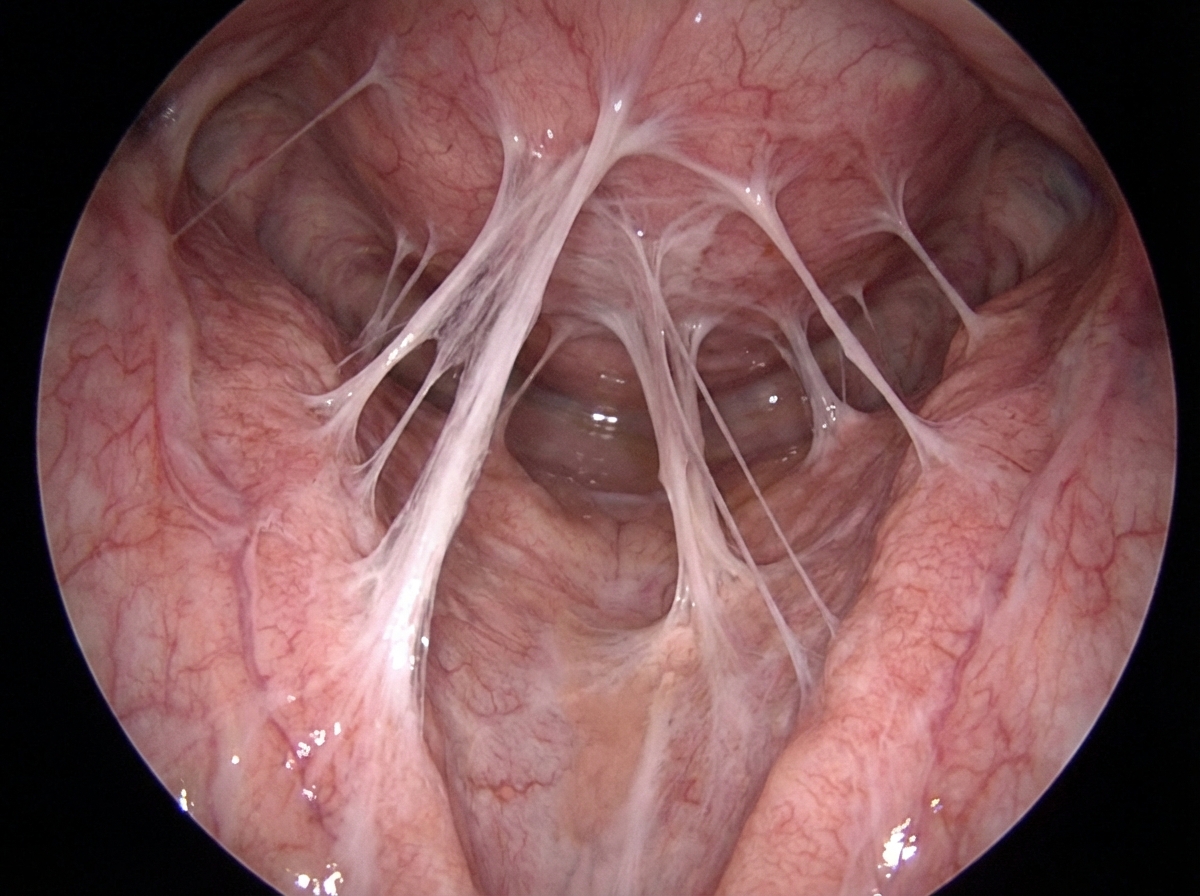
A 28-year-old woman and her husband are admitted to the office due to difficulties conceiving a child for the past year. Her menarche was at the age of 15 years, and her periods have been regular since then. Her medical history is positive for an abortion with curettage 5 years ago. A spermogram on the partner is performed, and it shows motile sperm cells. An ultrasound is performed on the patient and it is unremarkable. The laboratory results show that the FSH, LH, TSH, and prolactin levels are within normal ranges. A hysteroscopy is additionally performed and multiple adhesions are found in the uterus (refer to the image). Which of the following is the most likely composition of the scar tissue present in the uterus?
A previously healthy 29-year-old Taiwanese woman comes to the emergency department with vaginal bleeding and pelvic pressure for several hours. Over the past 2 weeks, she had intermittent nausea and vomiting. A home urine pregnancy test was positive 10 weeks ago. She has had no prenatal care. Her pulse is 80/min and blood pressure is 150/98 mm Hg. Physical examination shows warm and moist skin. Lungs are clear to auscultation bilaterally. Her abdomen is soft and non-distended. Bimanual examination shows a uterus palpated at the level of the umbilicus. Her serum beta human chorionic gonadotropin concentration is 110,000 mIU/mL. Urine dipstick is positive for protein and ketones. Transvaginal ultrasound shows a central intrauterine mass with hypoechoic spaces; there is no detectable fetal heart rate. An x-ray of the chest shows no abnormalities. Which of the following is the most appropriate next step in management?
Practice by Chapter
Preterm labor management
Practice Questions
Premature rupture of membranes
Practice Questions
Chorioamnionitis
Practice Questions
Abnormal labor patterns
Practice Questions
Shoulder dystocia management
Practice Questions
Umbilical cord prolapse
Practice Questions
Malpresentations (breech, face, brow)
Practice Questions
Trial of labor after cesarean
Practice Questions
Uterine rupture
Practice Questions
Placental abruption
Practice Questions
Placenta previa
Practice Questions
Amniotic fluid embolism
Practice Questions
Fetal heart rate abnormalities
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app