
Labor Complications — MCQs

On this page
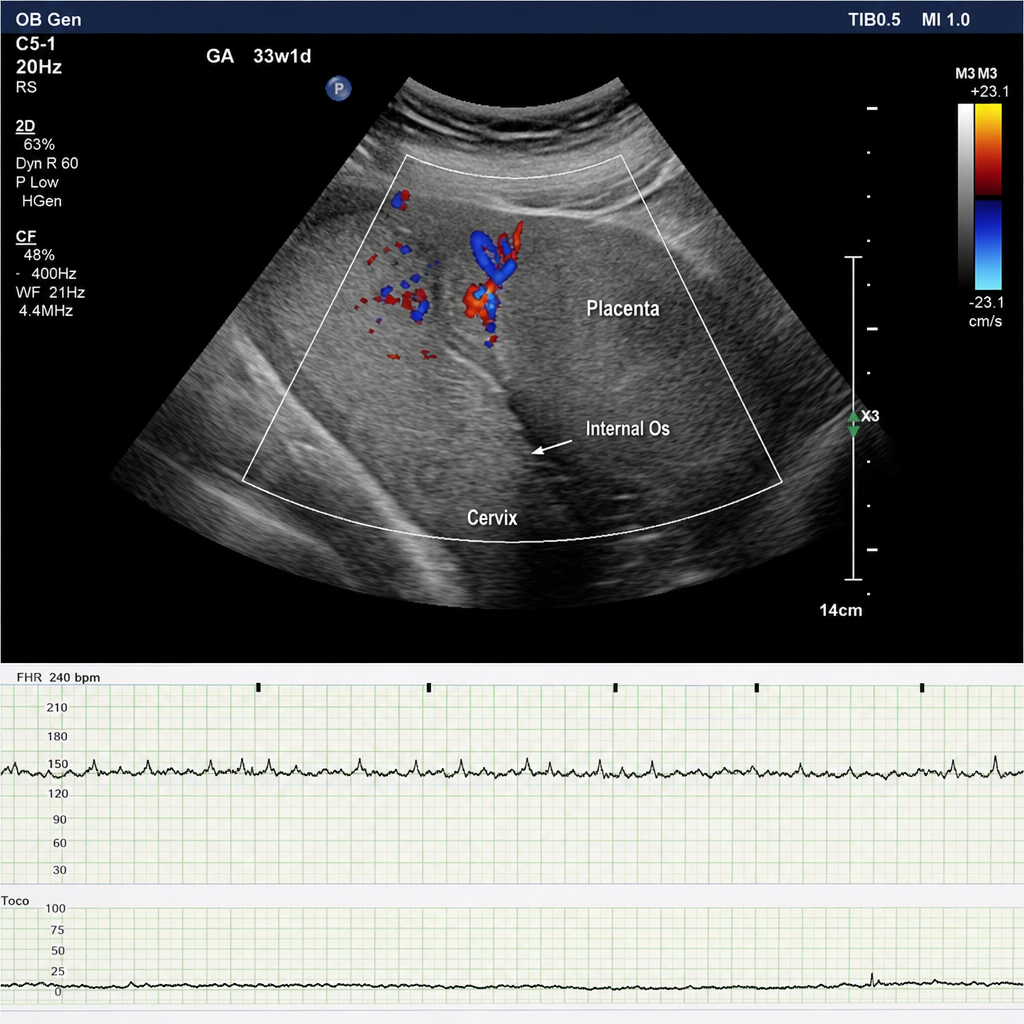
A 34-year-old G2P1 woman at 33 weeks of gestation presents with a 2-hour history of painless bright red vaginal bleeding. She denies contractions or fluid leakage. Vital signs: BP 112/70 mmHg, HR 88 bpm, O₂ saturation 99%. The fetal heart rate tracing shows a baseline of 140 bpm with moderate variability, accelerations present, and no decelerations — a reassuring pattern. Transabdominal ultrasound demonstrates the placenta completely covering the internal cervical os, consistent with complete placenta previa. Fetal biometry is consistent with 33 weeks. The patient is hemodynamically stable and the bleeding has slowed. Which of the following is the most appropriate next step in management?
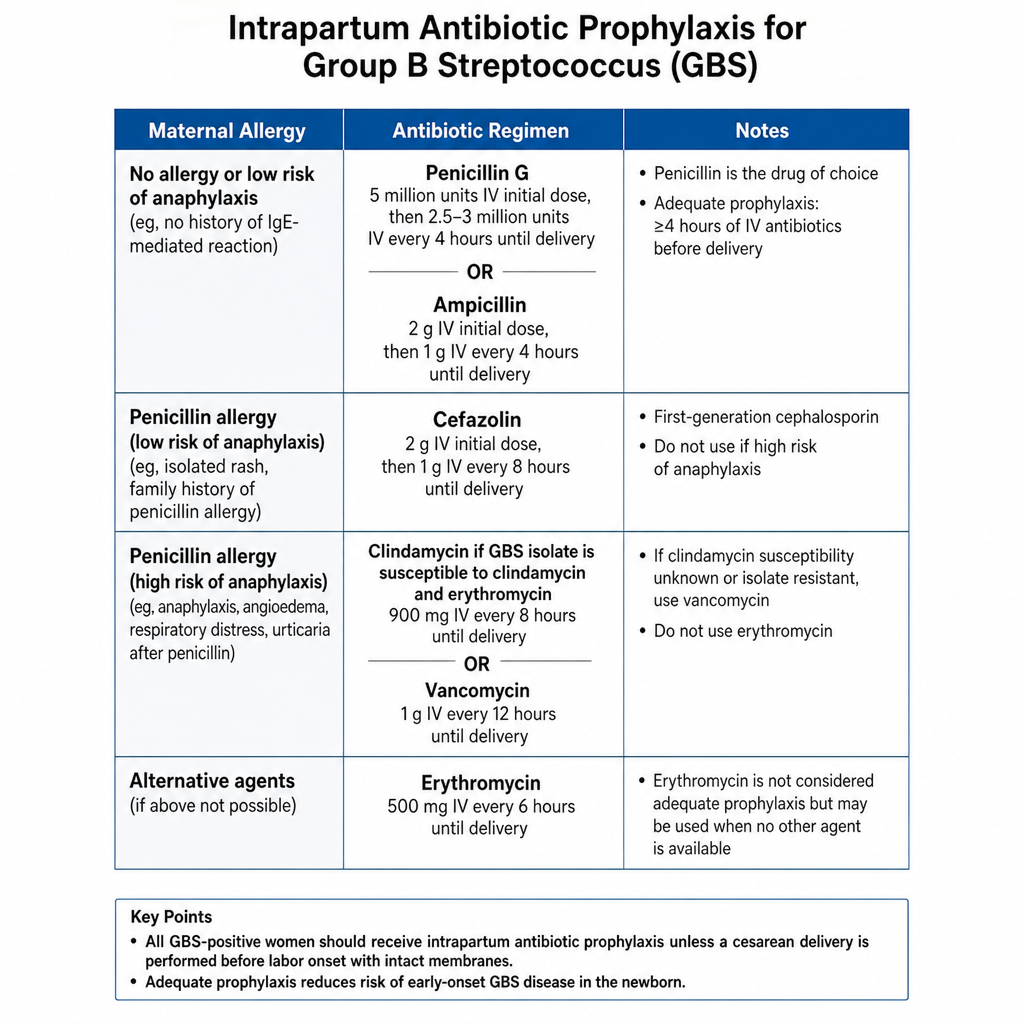
A 29-year-old G1P0 woman at 39 weeks of gestation is in active labor. She is GBS-positive per rectovaginal culture obtained at 36 weeks. She reports a penicillin allergy described as diffuse urticaria and throat tightening after amoxicillin administration as a child. Sensitivity testing is not available. Fetal heart rate tracing is Category I, cervix is 5 cm dilated. Which of the following represents the most appropriate antibiotic regimen for intrapartum prophylaxis in this patient?
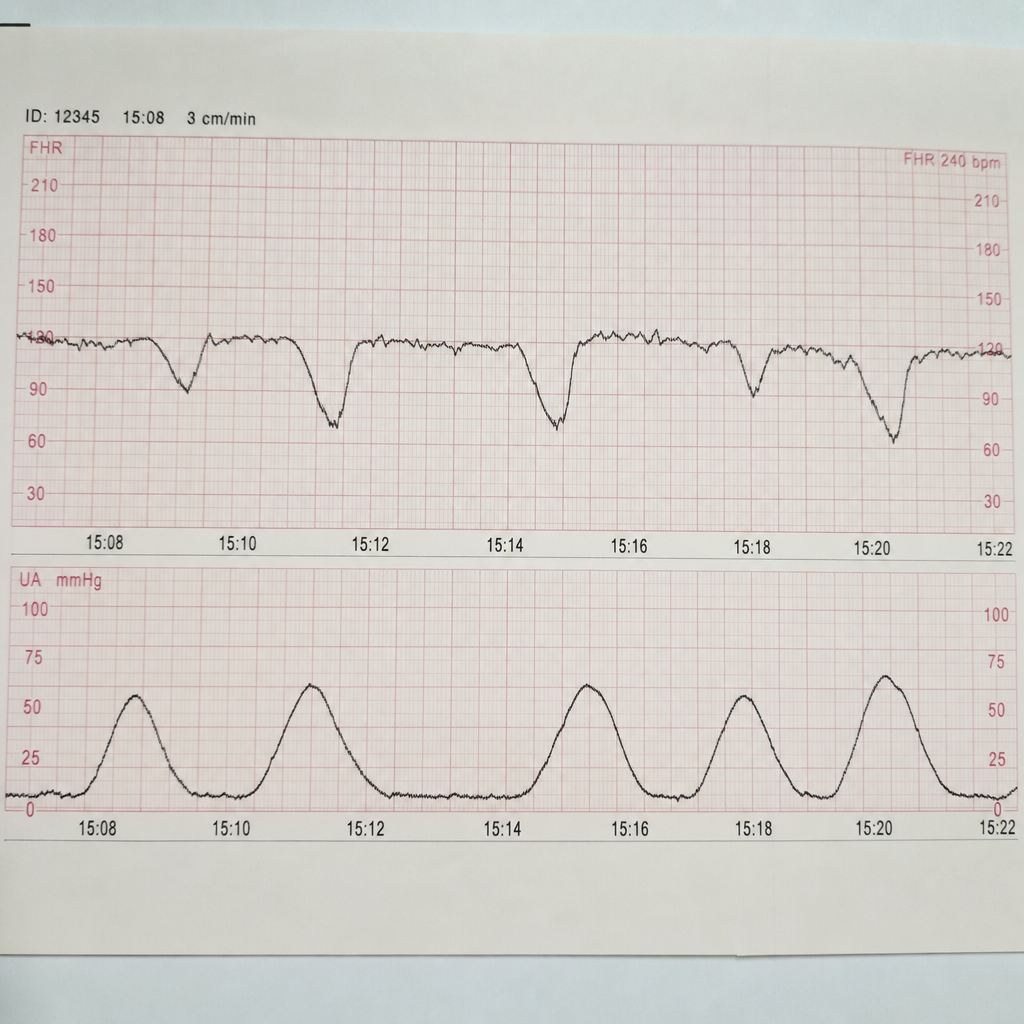
A 29-year-old woman, G1P0, at 40 weeks of gestation is in the second stage of labor. She has been pushing for 3 hours with an epidural in place. The fetal head is at +2 station, occiput anterior. The CTG strip shown demonstrates absent baseline variability with recurrent late decelerations, consistent with a Category III tracing. Maternal BP is 122/78 mmHg, temperature 37.1°C, and HR 88 bpm. The obstetric team is evaluating the tracing to determine the next course of action. Which of the following represents the most appropriate management?
A 32-year-old woman presents with a new 2 cm black nodular mass near her episiotomy scar. She reports that the mass is painful and tends to increase in size during menstruation. What is the most likely diagnosis?
A young woman presents with prolapse, and a mesh is being placed. Where is this mesh typically fixed to?
In fertility-preserving prolapse surgery, which bony landmark is used for suspension?
A patient with second-degree cervical prolapse complains of dribbling of urine when coughing. What is the most likely diagnosis?
A teenage patient presents with dysmenorrhea and chronic pelvic pain. Upon further investigation, she is found to have a transverse vaginal septum. What is the most likely diagnosis?
A 25-year-old primigravida is admitted to the hospital at 36 weeks gestation with a severe frontal headache. The initial assessment shows her vital signs to be as follows: blood pressure, 170/90 mm Hg; heart rate, 85/min; respiratory rate; 15/min; and temperature, 36.9℃ (98.4℉). The fetal heart rate is 159/min. The patient’s physical examination is remarkable for pitting edema of the lower extremity. Dipstick urine assessment shows 2+ proteinuria. While being evaluated the patient has a generalized tonic-clonic seizure. Which of the following pharmacologic agents should be used to control the seizures?
A 25-year-old primigravida is admitted to the hospital at 35 weeks gestation after she was hit in the abdomen by her roommate. She complains of severe dizziness, abdominal pain, and uterine contractions. Her vital signs are as follows: blood pressure 90/50 mm Hg, heart rate 99/min, respiratory rate 20/min, and temperature 36.3℃ (97.3℉). The fetal heart rate is 138/min. On examination, the patient is somnolent. There is an ecchymoses on the left side of her abdomen. The uterus is tender and strong uterine contractions are palpable. The fundus is between the xiphoid process and umbilicus There are no vaginal or cervical lesions and no visible bleeding. The cervix is long and closed. Which of the following findings would occur in this patient over time as her condition progresses?
Practice by Chapter
Preterm labor management
Practice Questions
Premature rupture of membranes
Practice Questions
Chorioamnionitis
Practice Questions
Abnormal labor patterns
Practice Questions
Shoulder dystocia management
Practice Questions
Umbilical cord prolapse
Practice Questions
Malpresentations (breech, face, brow)
Practice Questions
Trial of labor after cesarean
Practice Questions
Uterine rupture
Practice Questions
Placental abruption
Practice Questions
Placenta previa
Practice Questions
Amniotic fluid embolism
Practice Questions
Fetal heart rate abnormalities
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app