
High-risk pregnancies — MCQs

On this page
A 33-year-old nulliparous woman comes to the physician because of a 5-month history of increased flow and duration of her menses. Menses previously occurred at regular 32-day intervals and lasted 4 days with normal flow. They now last 10 days and the flow is heavy with the passage of clots. During this period, she has also had dyspareunia and cyclical lower abdominal pain. Her mother died of cervical cancer at the age of 58 years. Her BMI is 31 kg/m2. Her temperature is 37°C (98.6°F), pulse is 86/min, and blood pressure is 110/70 mm Hg. Pelvic examination shows an asymmetrically enlarged, nodular uterus consistent in size with a 12-week gestation. A urine pregnancy test is negative. Which of the following is the most likely cause of this patient's findings?
A 38-year-old primigravid woman at 34 weeks' gestation comes to the emergency department because of progressive shortness of breath for 3 hours. At a prenatal visit 2 weeks earlier, she was diagnosed with gestational hypertension. Amniocentesis with chromosomal analysis was performed at 16 weeks' gestation and showed no abnormalities. The patient has been otherwise healthy, except for a deep venous thrombosis 2 years ago that was treated with low molecular weight heparin. Her current medications include methyldopa and a multivitamin. She appears anxious. Her pulse is 90/min, respirations are 24/min, and blood pressure is 170/100 mm Hg. Crackles are heard over both lung bases. Pelvic examination shows a uterus consistent in size with a 32-week gestation. Examination of the heart, abdomen, and extremities shows no abnormalities. Which of the following is the most likely cause of this patient's shortness of breath?
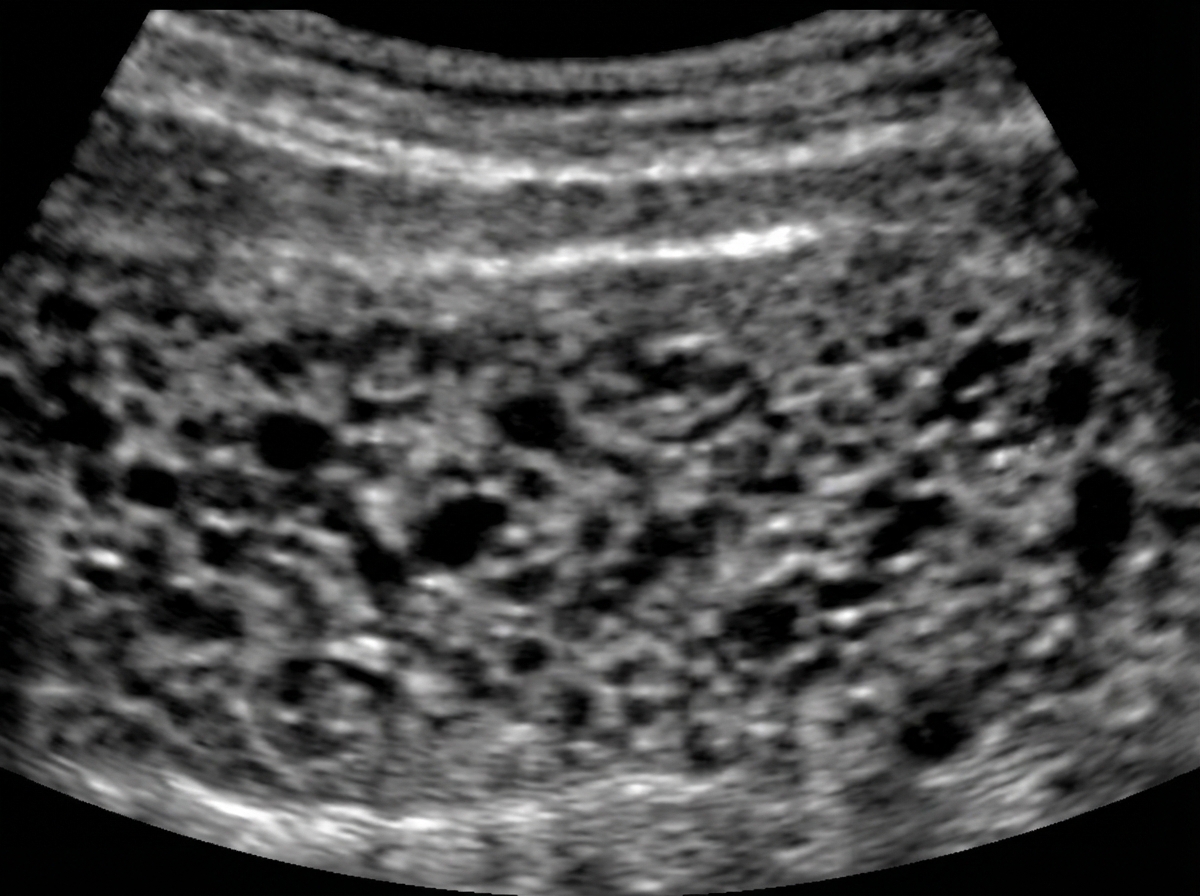
A 30-year-old woman comes to the primary care physician because she has felt nauseous and fatigued for 3 weeks. Menses occur at irregular 24- to 33-day intervals and last for 4–6 days. Her last menstrual period was 7 weeks ago. Her temperature is 37°C (98.6°F), pulse is 95/min, and blood pressure is 100/70 mm Hg. Pelvic examination shows an enlarged uterus. Her serum β-hCG concentration is 96,000 mIU/mL (N < 5). An abdominal ultrasound is shown. Which of the following is the most likely diagnosis?
A 22-year-old woman presents to the gynecologist for evaluation of amenorrhea and dyspareunia. The patient states that she recently got married and has been worried about getting pregnant. The patient states that she has never had a period and that sex has always been painful. On examination, the patient is Tanner stage 5 with no obvious developmental abnormalities. The vaginal exam is limited with no identified vaginal canal. What is the most likely cause of this patient’s symptoms?
A 57-year-old female presents to general gynecology clinic for evaluation of a pelvic mass. The mass was detected on a routine visit to her primary care doctor during abdominal palpation. In the office, she receives a transvaginal ultrasound, which reveals a mass measuring 11 cm in diameter. In the evaluation of this mass, elevation of which tumor marker would be suggestive of an ovarian cancer?
A 54-year-old woman comes to the physician because she has not had her menstrual period for the last 5 months. Menarche occurred at the age of 11 years, and menses occurred at regular 28-day intervals until they became irregular at 30- to 45-day intervals with light flow 2 years ago. She does not have vaginal dryness or decreased libido. She had four successful pregnancies and breastfed all her children until the age of 2 years. There is no personal or family history of serious illness. Except when she was pregnant, she has smoked one pack of cigarettes daily for 30 years. She does not drink alcohol. She is 167 cm (5 ft 5 in) tall and weighs 92 kg (203 lb); BMI is 33 kg/m2. Her vital signs are within normal limits. Physical examination shows no abnormalities. Which of the following best explains this patient's lack of symptoms other than amenorrhea?
A 20-year-old woman is brought to the emergency department 6 hours after the onset of colicky lower abdominal pain that has been progressively worsening. The pain is associated with nausea and vomiting. She has stable inflammatory bowel disease treated with 5-aminosalicylic acid. She is sexually active with her boyfriend and they use condoms inconsistently. She was diagnosed with chlamydia one year ago. Her temperature is 38.1°C (100.6°F), pulse is 94/min, respirations are 22/min, and blood pressure is 120/80 mm Hg. Examination shows right lower quadrant guarding and rebound tenderness. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
A 36-year-old G4P1021 woman comes to the emergency room complaining of intense abdominal pain and vaginal bleeding. She is 9 weeks into her pregnancy and is very concerned as she experienced similar symptoms during her past pregnancy losses. Her pain is described as “stabbing, 10/10 pain that comes and goes.” When asked about her vaginal bleeding, she reports that “there were some clots initially, similar to my second day of menstruation.” She endorses joint pains that is worse in the morning, “allergic” rashes at her arms, and fatigue. She denies weight loss, chills, fever, nausea/vomiting, diarrhea, or constipation. Physical examination reveals an enlarged and irregularly shaped uterus with a partially open external os and a flesh-colored bulge. Her laboratory findings are shown below: Serum: Hemoglobin: 11.8 g/dL Hematocrit: 35% Leukocyte count:7,600 /mm^3 with normal differential Platelet count: 200,000/mm^3 Bleeding time: 4 minutes (Normal: 2-7 minutes) Prothrombin time: 13 seconds (Normal: 11-15 seconds) Partial thromboplastin time (activated): 30 seconds (Normal: 25-40 seconds) What is the most likely cause of this patient’s symptoms?
A 43-year-old woman presents to her physician’s office complaining of fatigue and light headedness for one month. She has regular periods but notes that they have become heavier in the last year. She endorses increased urination and feels that she has gained weight in her abdomen, but review of systems is otherwise negative. She is a daycare teacher and has a first cousin with von Willebrand disease. Temperature is 98.4°F (36.9°C), pulse is 92/min, blood pressure is 109/72 mmHg, and respirations are 14/min. A CBC demonstrates: Hemoglobin: 9.9 g/dL Leukocyte count: 6,300/mm^3 Platelet count: 180,000/mm^3 Which of the following is the best next step to evaluate the etiology of this patient’s findings?
A 23-year-old G1P0 primigravid woman at 28 weeks estimated gestational age presents for a prenatal checkup. She says she has been having occasional headaches but is otherwise fine. The patient says she feels regular fetal movements and mild abdominal pain at times. Her past medical history is unremarkable. Current medications are a prenatal multivitamin and the occasional acetaminophen. Her blood pressure is 148/110 mm Hg today. On her last visit at 24 weeks of gestation, her blood pressure was 146/96 mm Hg. On physical exam, the fundus measures 28 cm above the pubic symphysis. Laboratory findings are significant for the following: Serum Glucose (fasting) 88 mg/dL Sodium 142 mEq/L Potassium 3.9 mEq/L Chloride 101 mEq/L Serum Creatinine 0.9 mg/dL Blood Urea Nitrogen 10 mg/dL Alanine aminotransferase (ALT) 18 U/L Aspartate aminotransferase (AST) 16 U/L Mean Corpuscular Volume (MCV) 85 fL Leukocyte count 4,200/mm3 Reticulocyte count 1% Erythrocyte count 5.1 million/mm3 Platelet count 95,000mm3 Urinalysis show: Proteins 2+ Glucose negative Ketones negative Leucocytes negative Nitrites negative Red Blood Cells (RBCs) negative Casts negative Which of the following medications would be the next best step in the treatment of this patient?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app