
High-risk pregnancies — MCQs

On this page
A 14-year-old girl is referred to a gynecologist for amenorrhea. Her mother is also concerned that she hasn't grown any hair "in her private parts." The patient states that she is getting used to high school and wants to join the volleyball team but complains that her weakness and headaches limit her physical activity. She does not share her mother's concerns about her menses. She reveals that her parents are maternal cousins. Her temperature is 98°F (37°C), blood pressure is 160/90 mmHg, pulse is 70/min, and respirations are 24/min. Her cardiac exam is unremarkable, and her abdominal exam reveals no bruits. After obtaining permission for a pelvic exam, the exam reveals a normal appearing vagina without any hair. No cervical os can be palpated. Initial labs reveal the following: Serum: Na+: 143 mEq/L Cl-: 110 mEq/L K+: 2.9 mEq/L HCO3-: 26 mEq/L BUN: 40 mg/dL Glucose: 104 mg/dL Creatinine: 1.3 mg/dL What is the most likely diagnosis?
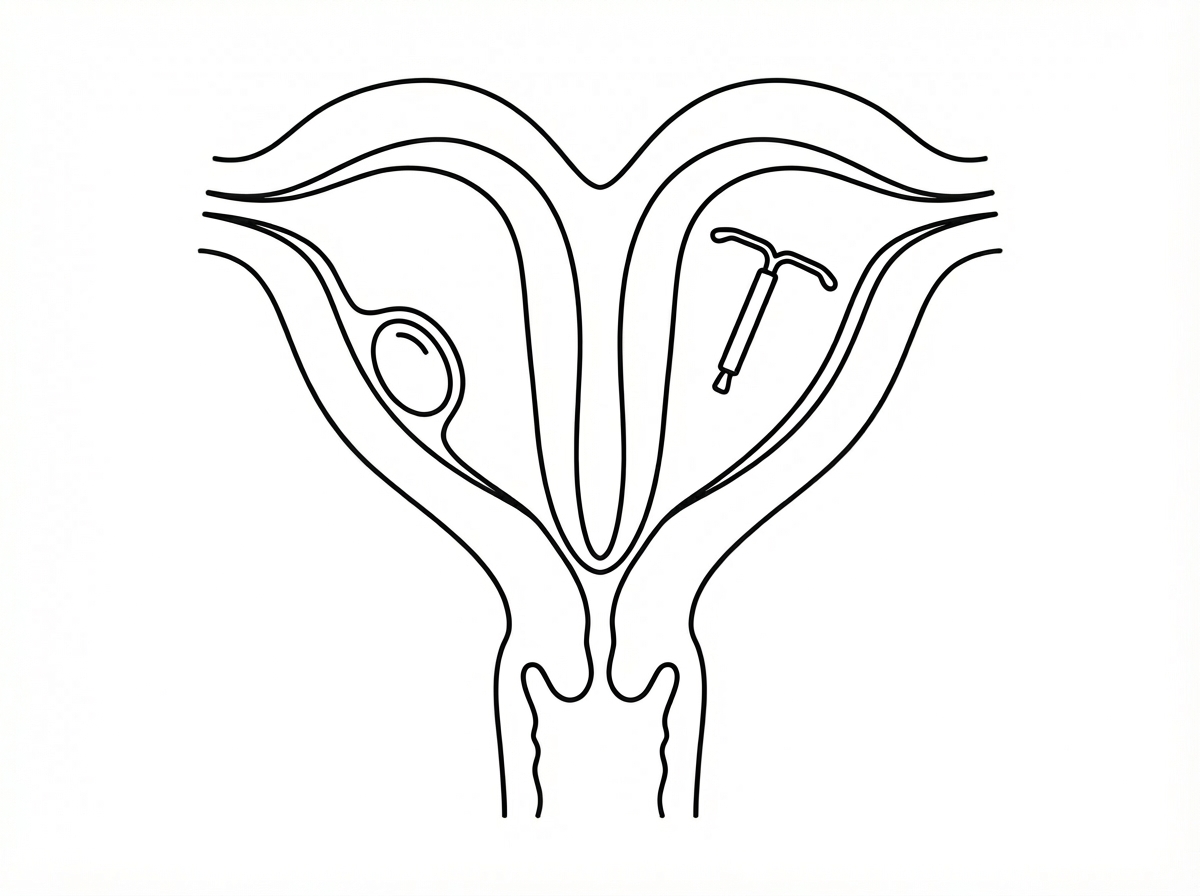
A 25-year-old woman whose menses are 2 weeks late, presents to her physician for evaluation. She also complains of fatigue, morning nausea, and mood changes. She is a nulliparous with previously normal menstrual cycles and no known medical conditions. She had an intrauterine device (IUD) placed 6 months ago. The patient’s vital signs are as follows: blood pressure 120/80 mm Hg, heart rate 72/min, respiratory rate 12/min, and temperature 36.5℃ (97.7℉). The physical examination is unremarkable. The gynecologic exam revealed cervical cyanosis and softening, uterine enlargement, and non-palpable adnexa. A transvaginal ultrasound examination is performed to check the IUD position. Ultrasonography revealed 2 uterine cavities; one cavity had a gestational sac and the intrauterine device was in the other uterine cavity. The cavities are fully separated but there is one cervix. What is the most likely etiology of this patient’s condition?
A 35-year-old woman comes to the physician because of a 3-month history of facial hair growth, acne, and irregular menses. Her friends have told her that her voice sounds lower than usual. Physical examination shows pustular acne and dark hair growth along the jawline. Serum studies show elevated testosterone levels and normal inhibin levels. An ultrasound of the pelvis shows a left-sided ovarian mass. Microscopic examination of the resected ovarian mass shows pale, testosterone-positive staining cells with cytoplasmic Reinke crystal inclusions. These abnormal cells are homologous to which of the following physiological cell type in females?
A 16-year-old girl is brought to the physician because she has not yet reached menarche. There is no personal or family history of serious illness. She is at the 20th percentile for weight and 50th percentile for height. Vital signs are within normal limits. Examination shows mild facial hair. There is no glandular breast tissue. Pubic hair is coarse and curly and extends to the inner surface of both thighs. Pelvic examination shows clitoromegaly. Ultrasound shows an absence of the uterus and ovaries. Which of the following is the most likely underlying cause for this patient's symptoms?
A 26-year-old woman, gravida 2, para 1, at 28 weeks' gestation comes to the physician for a prenatal visit. She feels well. Pregnancy and delivery of her first child were uncomplicated. Her temperature is 37.2°C (99°F) and blood pressure is 163/105 mm Hg. Her blood pressure 10 weeks ago was 128/84 mm Hg. At her last visit two weeks ago, her blood pressure was 142/92 mm Hg. Pelvic examination shows a uterus consistent in size with a 28-week gestation. A complete blood count and serum concentrations of electrolytes, creatinine, and hepatic transaminases are within the reference range. A urinalysis is within normal limits. Which of the following is the most appropriate next step in management?
A previously healthy 37-year-old woman, gravida 3, para 2, at 29 weeks' gestation comes to the physician because of colicky postprandial abdominal pain. Her vital signs are within normal limits. Physical examination shows a uterus consistent in size with a 29-week gestation. Ultrasonography of the abdomen shows multiple 5-mm hyperechoic masses within the gallbladder lumen. Which of the following processes is most likely involved in the pathogenesis of this patient's condition?
A 66-year-old woman presents to her primary care physician for a wellness exam. She noticed mild spotting a few days prior to presentation. Her last menstrual period was when she was 53 years of age, and she denies any trauma to the area. She is sexually active with one male partner and does not use condoms. Medical history is significant for type II diabetes mellitus and hypertension. She is currently taking metformin and lisinopril. Her last pap smear was normal. She is 5 ft 5 in (165.1 cm), weighs 185 lbs (84 kg), and BMI is 30.8 kg/m2. Her blood pressure is 115/70 mmHg, pulse is 85/min, and respirations are 15/min. Pelvic examination demonstrates a normal sized uterus with no adnexal masses. There are no vulvar, vaginal, or cervical lesions. Stool testing for blood is negative and an endometrial biopsy is performed, which demonstrates simple endometrial hyperplasia without atypia. Which of the following is the best next step in management?
A 42-year-old woman presents to her primary care physician for a checkup. She has been trying to get pregnant with her husband for the past 12 months but has been unsuccessful. The patient states that they have been having unprotected intercourse daily during this time frame. She states that she experiences her menses every 28 days. Her husband has 2 children from another marriage. Otherwise, the patient only complains of mild vaginal dryness during intercourse. The patient's past medical history is notable for seasonal allergies for which she takes loratadine and a chlamydial infection which was treated in college. On physical exam, you note a healthy woman. Cardiopulmonary, abdominal, and pelvic exam are within normal limits. Which of the following is the most likely diagnosis in this patient?
A 32-year-old primigravid woman with a history of seizures comes to the physician because she had a positive pregnancy test at home. Medications include valproic acid and a multivitamin. Physical examination shows no abnormalities. A urine pregnancy test is positive. Her baby is at increased risk for requiring which of the following interventions?
A 36-year-old primigravid woman at 22 weeks' gestation comes to the physician for a routine prenatal visit. Her previous prenatal visits showed no abnormalities. She has hyperthyroidism treated with methimazole. She previously smoked one pack of cigarettes daily for 15 years but quit 6 years ago. She reports gaining weight after quitting smoking, after which she developed her own weight loss program. She is 168 cm (5 ft 6 in) tall and weighs 51.2 kg (112.9 lb); BMI is 18.1 kg/m2. Her temperature is 37°C (98.5°F), pulse is 88/min, and blood pressure is 115/72 mm Hg. Pelvic examination shows no abnormalities. The fundus is palpated between the symphysis and the umbilicus. Ultrasound shows a fetal head at the 20th percentile and the abdomen at the 9th percentile. Fetal birth weight is estimated at the 9th percentile and a decreased amniotic fluid index is noted. The maternal quadruple screening test was normal. Thyroid-stimulating hormone is 0.4 mIU/mL, triiodothyronine (T3) is 180 ng/dL, and thyroxine (T4) is 10 μg/dL. Which of the following is the strongest predisposing factor for the ultrasound findings in this patient?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app