
High-risk pregnancies — MCQs

On this page
A 45-year-old woman presents with gradual abdominal distension that has progressively increased over the past 3 months. The physical examination showed shifting dullness. A paracentesis showed malignant cells. An ultrasound shows an adnexal mass. Which is the most likely cause of this condition?
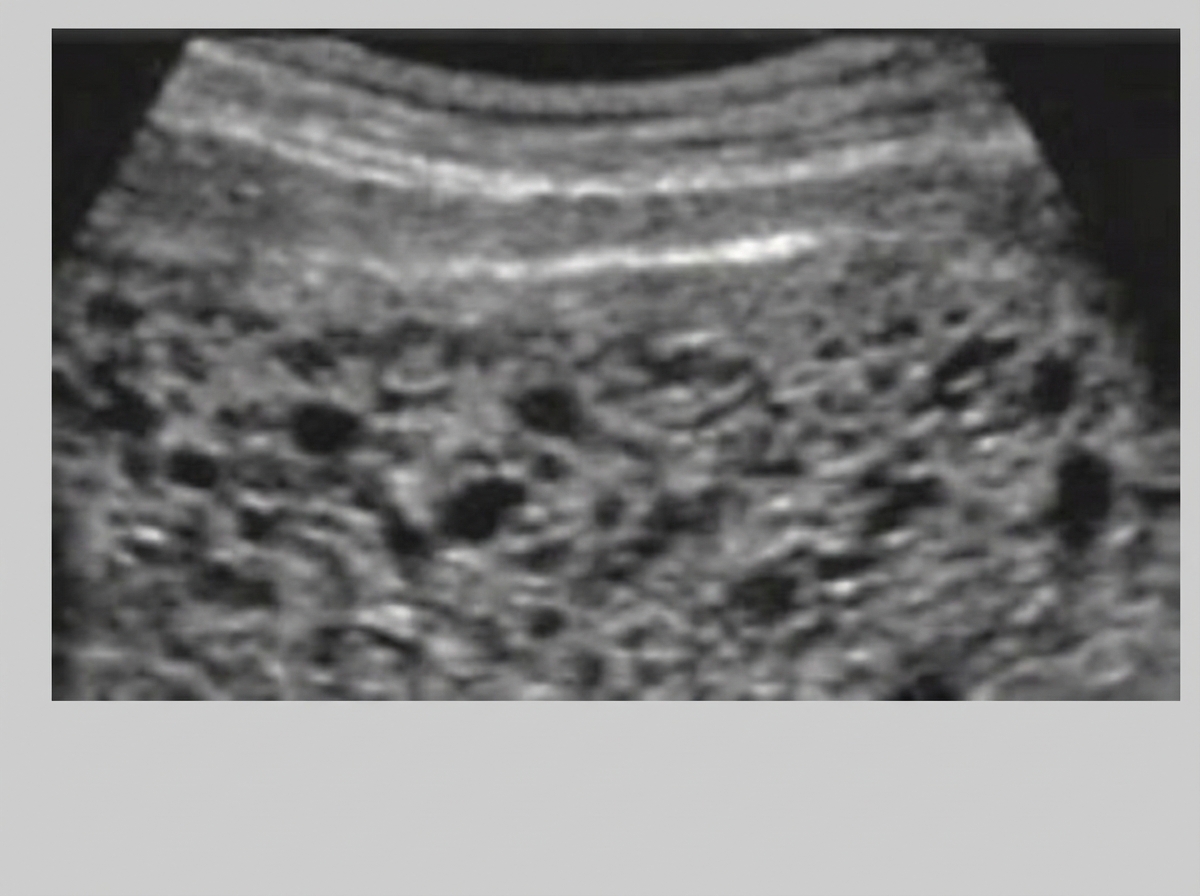
A 31-year-old Asian woman presents with painless vaginal bleeding late in the first trimester of her pregnancy. She has had no prenatal care up to this point. Serum HCG levels are elevated much more than expected. An abdominal ultrasound reveals findings consistent with a complete molar pregnancy, as shown in figure A. Which of the following is the most likely karyotype associated with this condition?
A 34-year-old woman comes to the physician for a routine health maintenance examination. She has gastroesophageal reflux disease. She recently moved to a new city. Her father was diagnosed with colon cancer at age 46. Her father's brother died because of small bowel cancer. Her paternal grandfather died because of stomach cancer. She takes a vitamin supplement. Current medications include esomeprazole and a multivitamin. She smoked one pack of cigarettes daily for 6 years but quit 2 years ago. She drinks one to two alcoholic beverages on weekends. She appears healthy. Vital signs are within normal limits. Physical examination shows no abnormalities. Colonoscopy is unremarkable. Germline testing via DNA sequencing in this patient shows mutations in DNA repair genes MLH1 and MSH2. Which of the following will this patient most likely require at some point in her life?
A 37-year-old G1P000 presents to her obstetrician for her first prenatal visit. She states that her last menstrual period (LMP) was 11 weeks ago, though she is unsure of the exact date as her periods are sometimes irregular. She and her husband had 5 months of timed, unprotected intercourse before she had a positive home pregnancy test 2 weeks ago. She has been feeling generally well but notes some morning nausea and vomiting. She also mentions that for the last 6 months or so, she has felt increasing pelvic pressure and worsening urinary frequency but has not sought medical care for these symptoms. The patient has a history of obesity and hypertension but is not on any medications. Her mother had a hysterectomy at age 64 for fibroids, and her sister had a twin pregnancy after assisted reproduction. At this visit, the patient’s temperature is 98.3° F (36.8° C), blood pressure is 142/85 mmHg, pulse is 82/min, and respirations are 14/min. She has gained 4 pounds since the last time she weighed herself 4 months ago. On exam, the patient’s fundus is palpated at the umbilicus, her cervix is closed and firm, and there are no adnexal masses. Her lab results are shown below: ß-hCG: 81,324 mIU/mL Thyroid stimulating hormone (TSH): 1.2 µIU/L Which of the following is the most likely diagnosis?
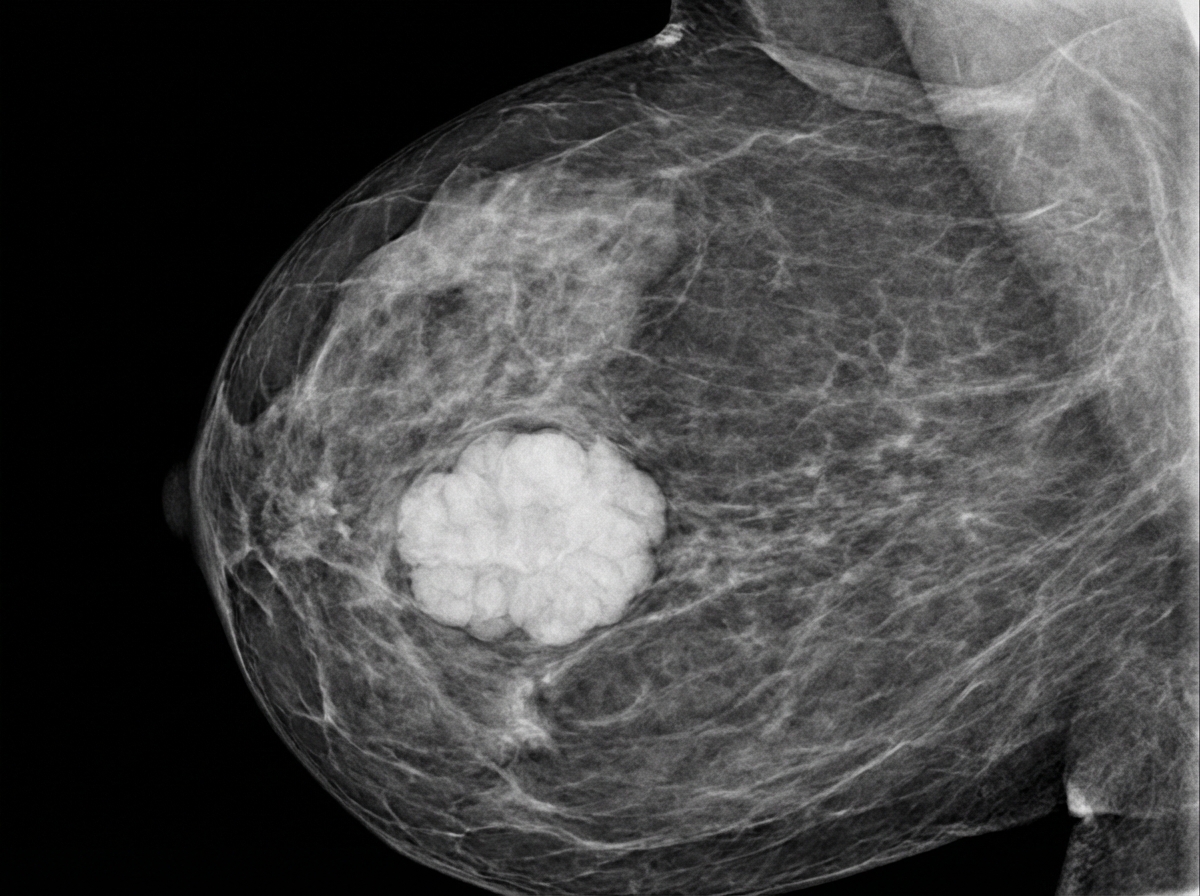
A 39-year-old female presents to her gynecologist complaining of a breast lump. Two weeks ago, while performing a breast self-examination she noticed a small firm nodule in her left breast. She is otherwise healthy and takes no medications. Her family history is notable for a history of breast cancer in her mother and maternal aunt. On physical examination, there is a firm immobile nodular mass in the superolateral quadrant of her left breast. A mammogram of her left breast is shown. Genetic analysis reveals a pathogenic BRCA1 mutation on chromosome 17q21. Which histopathologic pattern of breast carcinoma is most particularly associated with BRCA1 mutations?
A 27-year-old woman presents to her obstetrician for a regular follow-up appointment. The patient is 32 weeks pregnant. She has been followed throughout her pregnancy and has been compliant with care. The patient has a past medical history of a seizure disorder which is managed with valproic acid as well as anaphylaxis when given IV contrast, penicillin, or soy. During the patient's pregnancy she has discontinued her valproic acid and is currently taking prenatal vitamins, folic acid, iron, and fish oil. At this visit, results are notable for mild anemia, as well as positive findings for an organism on darkfield microscopy. The patient is up to date on her vaccinations and her blood glucose is 117 mg/dL at this visit. Her blood pressure is 145/99 mmHg currently. Which of the following is the most appropriate management for this patient?
A 41-year-old nulliparous woman, at 15 weeks' gestation comes to the emergency department because of an 8-hour history of light vaginal bleeding. She had a spontaneous abortion at 11 weeks' gestation 9 months ago. Vital signs are within normal limits. Abdominal examination is unremarkable. On pelvic examination, there is old blood in the vaginal vault and at the closed cervical os. There are bilateral adnexal masses. Serum β-hCG concentration is 122,000 mIU/ml. Results from dilation and curettage show hydropic chorionic villi and proliferation of cytotrophoblasts and syncytiotrophoblasts. There are no embryonic parts. Vaginal ultrasound shows that both ovaries are enlarged and have multiple thin-walled, septated cysts with clear content. Which of the following is the most likely cause of the ovarian findings?
A 38-year-old woman, gravida 2, para 1, at 32 weeks' gestation comes to the physician for a prenatal visit. Pregnancy and delivery of her first child were uncomplicated. She has type 1 diabetes mellitus treated with insulin. Her temperature is 37.2°C (99°F), pulse is 92/min, respirations are 16/min, and blood pressure is 110/86 mm Hg. Examination shows minimal bilateral edema below the knees. The uterus is consistent in size with a 29-week gestation. The remainder of the examination shows no abnormalities. Transabdominal ultrasound shows an intrauterine pregnancy in longitudinal lie, normal fetal cardiac activity, an amniotic fluid index of 5 cm and calcifications of the placenta. This patient's child is at greatest risk of developing which of the following conditions?
A 16-year-old female presents to her pediatrician’s office because she has not yet started menstruating. On review of systems, she states that she has been increasingly tired, constipated, and cold over the last 6 months. She also endorses a long history of migraines with aura that have increased in frequency over the last year. She complains that these symptoms have affected her performance on the track team. She states that she is not sexually active. Her mother and sister both underwent menarche at age 15. The patient is 5 feet, 4 inches tall and weighs 100 pounds (BMI 17.2 kg/m^2). Temperature is 98.4°F (36.9°C), blood pressure is 98/59 mmHg, pulse is 98/min, and respirations are 14/min. On exam, the patient appears pale and has thinning hair. She has Tanner stage IV breasts and Tanner stage III pubic hair. Which of the following would be most useful in determining this patient’s diagnosis?
A 43-year-old woman comes to the physician because of a 3-month history of increased flow and duration of her menses. Menses previously occurred at regular 28-day intervals and lasted 5 days with normal flow. They now last 8–9 days and the flow is heavy with the passage of clots. During this period, she has also had lower abdominal pain that begins 2–3 days prior to onset of her menses and lasts for 2 days after the end of her menses. She has three children. Her mother died of endometrial cancer at the age of 61 years. Her temperature is 37°C (98.6°F), pulse is 86/min, and blood pressure is 110/70 mm Hg. Pelvic examination shows a uniformly enlarged, boggy uterus consistent in size with an 8-week gestation that is tender on palpation. A urine pregnancy test is negative. Which of the following is the most likely cause of this patient's findings?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app