
High-risk pregnancies — MCQs

On this page
A 25-year-old woman comes to the physician because she has noted darkening of the skin around her neck since wearing a chain she recently bought at a thrift shop. The darkening occurred gradually over the past 2 months and is accompanied by thickening of the affected skin. She has peptic ulcer disease. Menses occur at irregular 35- to 60-day intervals and last for 9 days with heavy flow. Menarche was at the age of 14 years and her last menstrual period was 3 weeks ago. She is sexually active with her husband and they do not use contraception. The patient's only medication is cimetidine. She is 163 cm (5 ft 4 in) tall and weighs 91 kg (200 lb); BMI is 34 kg/m2. Vital signs are within normal limits. Physical examination shows velvety, hyperpigmented plaques in the axillae, the inframammary fold, and around the neck. The remainder of the examination shows no abnormalities. Further evaluation of this patient is most likely to show which of the following findings?
A 24-year-old woman at 36 weeks pregnant presents to the emergency department with a headache and abdominal pain. The woman has no known past medical history and has inconsistently followed up with an obstetrician for prenatal care. Her temperature is 98.5°F (36.9°C), blood pressure is 163/101 mmHg, pulse is 90/min, respirations are 16/min, and oxygen saturation is 97% on room air. Prior to performing the physical exam, the patient experiences a seizure, which resolves after 60 seconds. Which of the following is the best management for this patient?
A 45-year-old woman visits your office with concerns about recent changes in her menstrual cycle. She noticed that her menses last longer and are heavier, to the point of needing almost twice the number of sanitary pads than 6 months ago. She denies any abdominal or pelvic discomfort. She started menstruating at 9 years of age. She had a negative Pap smear and HPV test 5 years ago. The physical examination is unremarkable with no masses on abdominal palpation and the pelvic examination is negative for vaginal lesions or tenderness. The bimanual examination reveals a mobile, non-tender, retroverted uterus with no masses in the adnexa. A transvaginal ultrasound performed 4 days after her last menses revealed an endometrial thickness of 4 mm. Which of the following is the most likely cause of this patient’s condition?
A 36-year-old primigravida woman visits her gynecologist during the 28th week of her pregnancy. Physical examination reveals pitting edema around her ankles and elevated systolic blood pressure. 24-hour urine collection yields 4 grams of protein. If left untreated, the patient is most at increased risk for which of the following:
A 31-year-old G1P0000 presents to her obstetrician for her first prenatal visit after having a positive home pregnancy test one week ago. She states that her last menstrual period was 8 weeks ago. The patient has a past medical history of type I diabetes mellitus since childhood and is on insulin. Her hemoglobin A1c two weeks ago was 13.7%. At that time, she was also found to have microalbuminuria on routine urinalysis, and her primary care provider prescribed lisinopril but the patient has not yet started taking it. The patient’s brother is autistic, but family history is otherwise unremarkable. At this visit, her temperature is 98.6°F (37.0°C), blood pressure is 124/81 mmHg, pulse is 75/min, and respirations are 14/min. Exam is unremarkable. This fetus is at increased risk for which of the following?
A 36-year-old G1P0 Caucasian woman in her 12th week of pregnancy presents to her obstetrician with vaginal bleeding. She also reports 3 episodes of non-bloody, non-bilious emesis. She failed to show up for her last 2 pre-natal visits due to work. Her past medical history is notable for obesity and type I diabetes mellitus. Her family history is notable for ovarian cancer in her mother and endometrial cancer in her maternal grandmother. On examination, her uterus is at 16 weeks in size and she has mild tenderness to palpation on her right suprapubic region. A transvaginal ultrasound in this patient would most likely reveal which of the following?
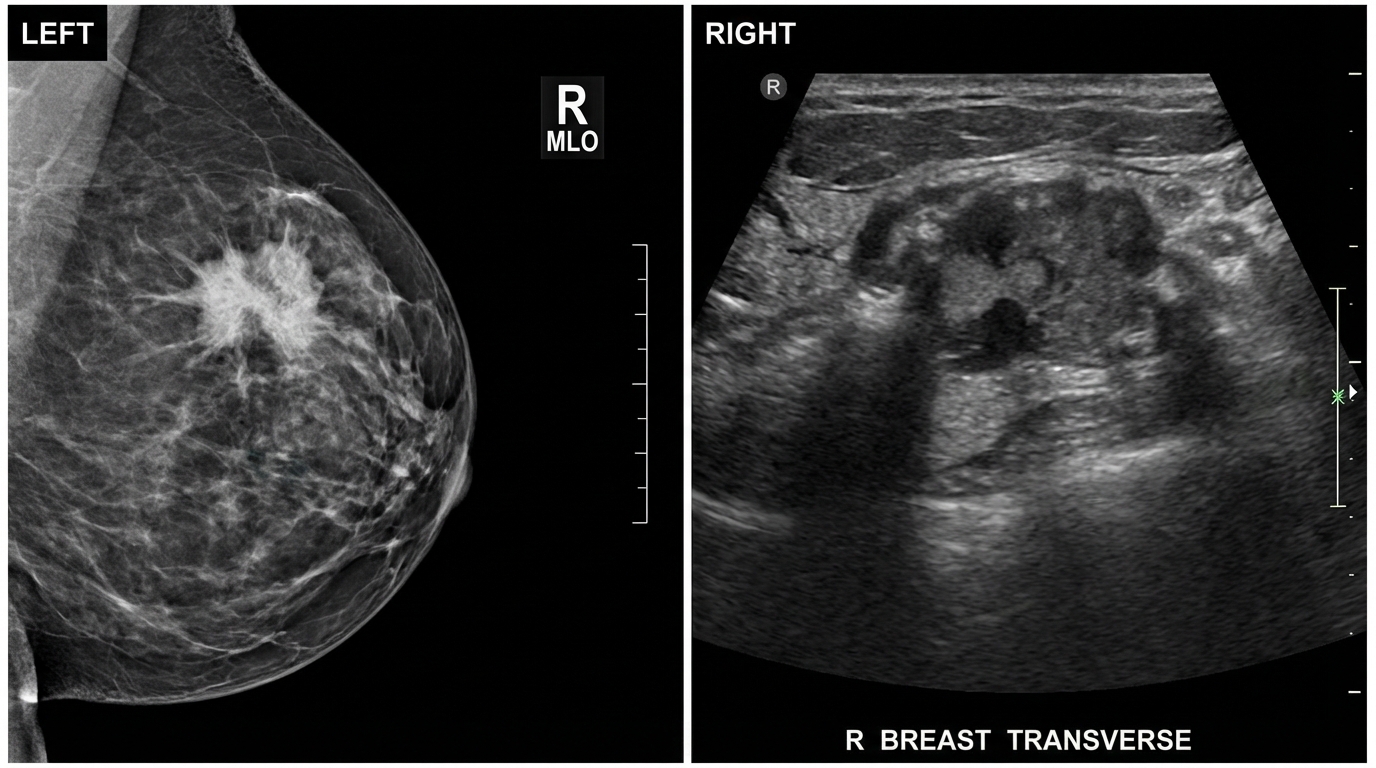
A 52-year-old G0P0 presents to her gynecologist for an annual exam. The patient notes that she recently felt a lump in her right breast, and it has persisted for several months. She has not noticed any abnormal breast discharge or skin changes, and the lump is not particularly tender. The patient also reports feeling especially sweaty in the last three months and occasionally having sudden heat waves. As a result, she has been increasing her use of antiperspirant in the axilla. The patient has no medical problems, has a BMI of 18.4 kg/m^2, and takes no medications. She underwent menarche at age 16 and had a levonorgestrel intrauterine device inserted three years ago due to heavy menstrual bleeding. The patient has now been amenorrheic for two years. She has a family history of breast cancer in her cousin at age 61 and hypertension in her father, who is 91. At this office visit, a 3x3 cm lump is palpated in the upper outer quadrant of the right breast. It is firm and not freely mobile. Ultrasound and mammogram are shown in Figures A and B. Which feature in this patient's history increases her risk for this condition?
A 26-year-old primigravid woman at 25 weeks' gestation comes to the physician for a prenatal visit. She has no history of serious illness and her only medication is a daily prenatal vitamin. A 1-hour 50-g glucose challenge shows a glucose concentration of 167 mg/dL (N < 135). A 100-g oral glucose tolerance test shows glucose concentrations of 213 mg/dL (N < 180) and 165 mg/dL (N < 140) at 1 and 3 hours, respectively. If she does not receive adequate treatment for her condition, which of the following complications is her infant at greatest risk of developing?
A 23-year-old primigravid woman comes to the physician at 28 weeks' gestation for a prenatal visit. Over the past 2 months, she has developed a hoarse voice and facial hair. Her medications include iron and a multivitamin. The last fetal ultrasonography, performed at 21 weeks' gestation, was unremarkable. Vital signs are within normal limits. Examination shows facial acne and hirsutism. Pelvic examination shows clitoromegaly. The uterus is consistent in size with a 28-week gestation. There are bilateral adnexal masses present on palpation. Ultrasonography shows a single live intrauterine pregnancy consistent with a 28-week gestation and bilateral 6-cm solid, multinodular ovarian masses. Serum androgen levels are increased. Which of the following is the most appropriate next step in management?
A 25-year-old G1P0 at 20 weeks of gestation woman arrives at a prenatal appointment complaining of pelvic pressure. She has had an uncomplicated pregnancy thus far. She takes prenatal vitamins and eats a well-balanced diet. Her medical history is significant for major depressive disorder that has been well-controlled on citalopram. Her mother had gestational diabetes with each of her 3 pregnancies. On physical exam, the cervix is soft and closed with minimal effacement. There is white vaginal discharge within the vagina and vaginal vault without malodor. Vaginal pH is 4.3. A transvaginal ultrasound measures the length of the cervix as 20 mm. Which of the following is most likely to prevent preterm birth in this patient?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app