
High-risk pregnancies — MCQs

On this page
A 32-year-old G1P0 woman presents to the emergency department at 34 weeks gestation. She complains of vague upper abdominal pain and nausea which has persisted for 2 weeks, as well as persistent headache over the past several days. Her temperature is 99.0°F (37.2°C), blood pressure is 164/89 mmHg, pulse is 88/min, respirations are 19/min, and oxygen saturation is 98% on room air. Hemoglobin: 10 g/dL Hematocrit: 30% Leukocyte count: 7,800/mm^3 with normal differential Platelet count: 25,000/mm^3 Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.1 mg/dL Ca2+: 10.2 mg/dL AST: 199 U/L ALT: 254 U/L Urine: Color: Yellow Protein: Positive Blood: Positive The patient begins seizing. Which of the following is the most appropriate definitive treatment for this patient?
A 22-year-old female presents at 24 weeks gestation with a chief complaint of burning upon urination. On physical exam, you note a gravid uterus that extends above the umbilicus. A urine analysis and culture is sent demonstrating over 100,000 colony forming units of E. coli. Of note this patient had a similar UTI 7 weeks ago that was resolved with appropriate medication. Which of the following is the most appropriate management of this patient?
A 30-year-old primigravida schedules an appointment with her obstetrician for a regular check-up. She says that everything is fine, although she reports that her baby has stopped moving as much as previously. She is 22 weeks gestation. She denies any pain or vaginal bleeding. The obstetrician performs an ultrasound and also orders routine blood and urine tests. On ultrasound, there is no fetal cardiac activity or movement. The patient is asked to wait for 1 hour, after which the scan is to be repeated. The second scan shows the same findings. Which of the following is the most likely diagnosis?
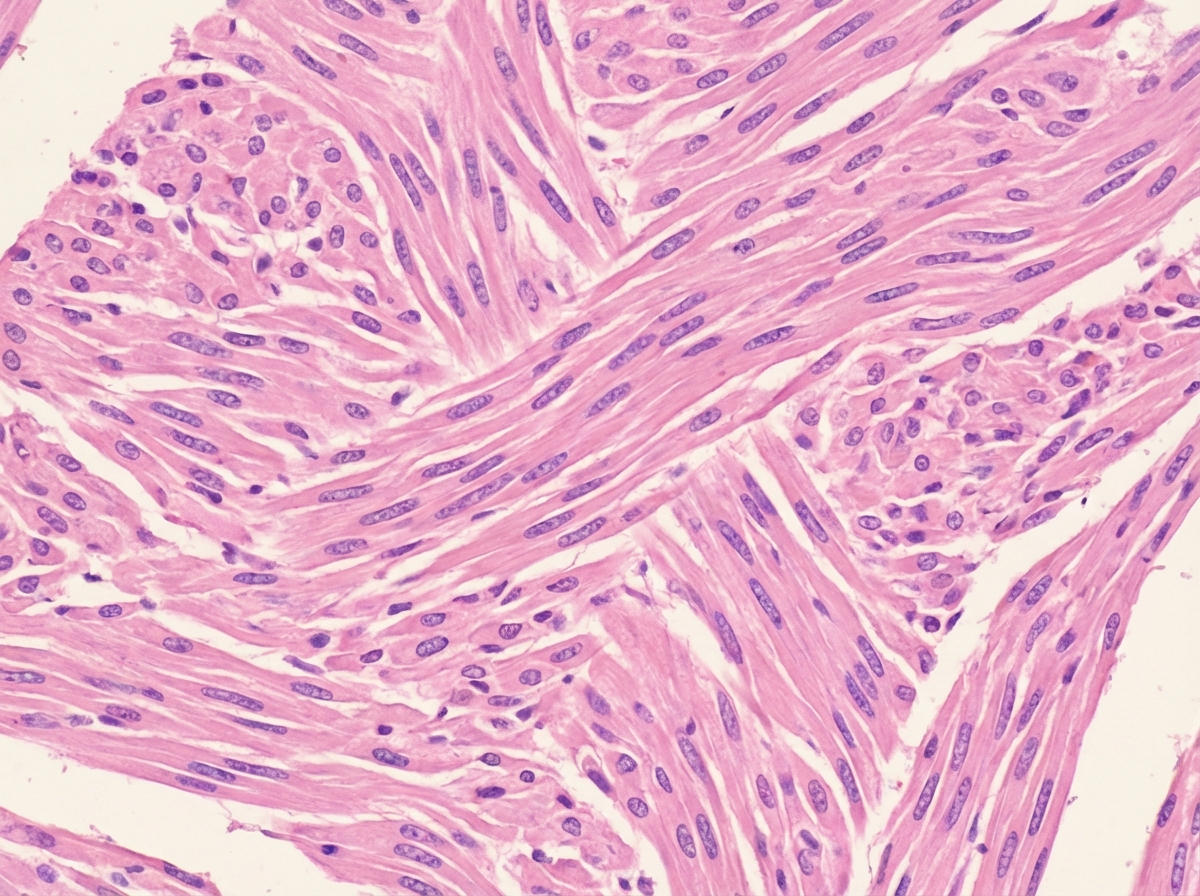
A 37-year-old nulliparous woman comes to the physician because of a 6-month history of heavy, prolonged bleeding with menstruation, dyspareunia, and cyclical abdominal pain. Menses previously occurred at regular 28-day intervals and lasted 4 days with normal flow. Pelvic examination shows an asymmetrically enlarged, nodular uterus consistent in size with a 10-week gestation. A urine pregnancy test is negative. A photomicrograph of a section of a biopsy or excision specimen from a uterine mass is shown. Which of the following is the most likely diagnosis?
A 19-year-old woman comes to the physician because of pelvic pain and vaginal discharge that began 2 days ago. She has no history of serious medical illness and takes no medications. Her temperature is 39°C (102.2°F). Pelvic examination shows pain with movement of the cervix and mucopurulent cervical discharge. A Gram stain of the discharge does not show any organisms. A Giemsa stain shows intracytoplasmic inclusions. The patient's current condition puts her at increased risk for which of the following complications?
A 33-year-old G1P0 at 32 weeks gestation presents to her OB/GYN for a prenatal check-up. Her medical history is significant for type II pregestational diabetes mellitus, which has been well-controlled with diet and insulin so far throughout her pregnancy. Which of the following is the recommended future follow-up for this patient?
A 26-year-old woman with a history of asthma presents to the emergency room with persistent gnawing left lower quadrant abdominal pain. She first noticed the pain several hours ago and gets mild relief with ibuprofen. She has not traveled recently, tried any new foods or medications, or been exposed to sick contacts. She is sexually active with her boyfriend and admits that she has had multiple partners in the last year. Her temperature is 99.5°F (37.5°C), blood pressure 77/45 mmHg, pulse is 121/min, and respirations are 14/min. On exam, she appears uncomfortable and diaphoretic. She has left lower quadrant tenderness to palpation, and her genitourinary exam is normal. Her urinalysis is negative and her pregnancy test is positive. Which of the following would be the appropriate next step in management?
A 28-year-old woman comes to a fertility clinic because she has been trying to conceive for over a year without success. She has never been pregnant, but her husband has 2 children from a previous marriage. She broke a collarbone during a skiing accident but has otherwise been healthy with no chronic conditions. On physical exam, she is found to have minimal pubic hair and suprapubic masses. Speculum examination reveals a small vagina with no cervical canal visible. The most likely cause of this patient's infertility has which of the following modes of inheritance?
A 26-year-old G6P1050 presents for evaluation of infertility. She and her husband have been trying to have a child for the past three years. Over that time period, the patient suffered five miscarriages. Her past medical history is significant for anemia, bipolar disorder, and a blood clot in her right lower extremity that occurred during her first pregnancy. The patient reports she has been feeling fatigued and has gained at least 10 pounds within the last two months. She often cries when she thinks about the miscarriages and has trouble falling asleep at night. She admits that while she had quit smoking during the pregnancy of her first child, and one month after the birth she started smoking again. She currently smokes about a half a pack of cigarettes a day. A review of systems is also positive for diffuse joint discomfort. The patient's current medications include minocycline for acne, and prenatal vitamins. A physical exam is unremarkable. Her temperature is 99°F (37.2°C), pulse is 72/minute, blood pressure is 118/78 mmHg, and oxygen saturation is 98% O2 on room air. Routine labs are drawn, as shown below: Leukocyte count: 6,500/mm^3 Platelet count: 210,000/mm^3 Hemoglobin: 11.0 g/dL Prothrombin time: 12 seconds Activated partial thromboplastin time: 43 seconds International normalized ratio: 1.1 Which of the following is associated with this patient’s infertility?
A 34-year-old G3P2 is admitted to the hospital at 32 weeks gestation with vaginal bleeding, which started 4 hours ago when she was taking a nap. She reports no pain or uterine contractions. The course of the current pregnancy has been uncomplicated. The two previous pregnancies resulted in cesarean sections. She did not undergo a scheduled ultrasound examination at 20 weeks gestation . Her vital signs are as follows: blood pressure, 110/60 mm Hg; heart rate, 77/min; respiratory rate, 14/min; and temperature, 36.6℃ (97.9℉). The fetal heart rate is 147/min. On examination, abdominal palpation is significant for normal uterine tone and no tenderness. The perineum is moderately bloody. The patient continues to pass a small amount of blood. Which of the following investigations would be most likely to confirm the diagnosis?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app