
High-risk pregnancies — MCQs

On this page
A husband requests paternity testing for his twins. The results show that one twin is biologically his child, but the other twin is not. What is the most likely diagnosis?
A patient presents with cannonball lesions in the lungs following a recent molar pregnancy evacuation. What is the most appropriate management?
An elderly female presented with dribbling of urine only on coughing and straining. What type of urinary incontinence is she suffering from
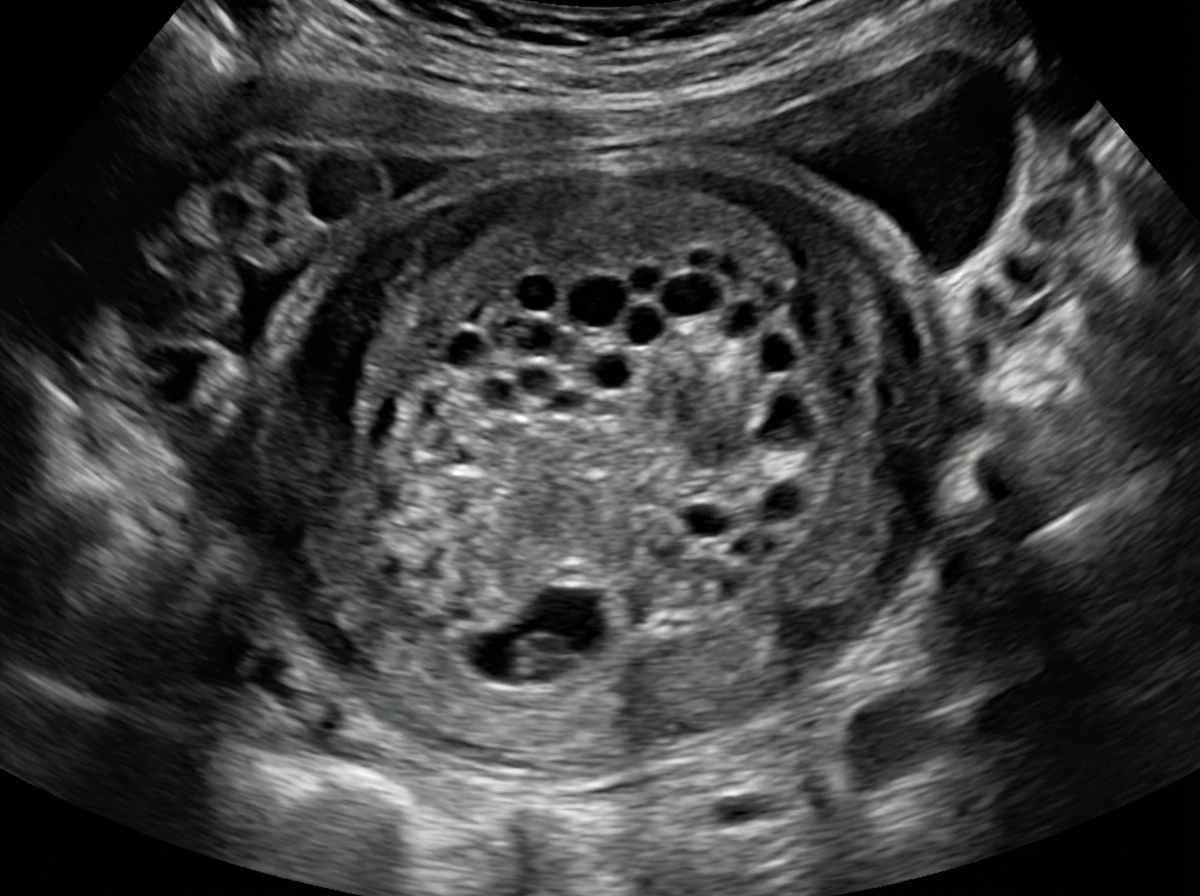
A 26-year-old primigravid woman comes to the emergency department because of a 10-hour history of vaginal bleeding and lower abdominal pain. She also had nausea and fatigue for the past 4 weeks. Her last menstrual period was 9 weeks ago. There is no history of medical illness. Vital signs are within normal limits. Pelvic examination shows a uterus consistent in size with a 9-week gestation. A urine pregnancy test is positive. β-HCG level is 108,000 mIU/mL (N < 5 mIU/mL). Transvaginal ultrasonography shows unclear, amorphous fetal parts and a large placenta with multiple cystic spaces. Which of the following is the most likely cause of this patient's condition?
A 27-year-old woman seeks an evaluation from her gynecologist complaining of vaginal discharge. She has been sexually active with 3 partners for the past year. Recently, she has been having pain during intercourse. Her temperature is 37.2°C (99.1°F), the blood pressure is 110/80 mm Hg, and the pulse is 78/min. The genital examination is positive for cervical motion tenderness. Even with treatment, which of the following complications is most likely to occur later in this patient's life?
A 32-year-old woman presents to her gynecologist’s office complaining of increasing fatigue. She mentions that she has been feeling this way over the past few months especially since her menstrual periods started becoming heavier than usual. She denies any abdominal pain, except for cramps during menstruation which are sometimes severe. She has never required medical care in the past except for occasional bouts of flu. She mentions that she is very tired even after a good night's sleep and is unable to do anything around the house once she returns from work in the evening. There are no significant findings other than conjunctival pallor. Her blood test results show a hemoglobin level of 10.3 g/dL, hematocrit of 24%, ferritin of 10 ng/mL and a red cell distribution width of 16.5%. Her peripheral blood smear is shown in the picture. Which of the following is the next best step in the management of this patient?
A 30-year-old G3P1011 seeks evaluation at the obstetrics clinic for lower abdominal pain and vaginal bleeding. She is 15 weeks pregnant based on a first-trimester ultrasound. She had spotting early in the pregnancy, but has had no other problems. On physical examination she appears mildly anxious. Her vital signs are normal except for a heart rate of 120 beats a minute. No abdominal tenderness is elicited. The cervical os is closed with a small amount of blood pooling in the vagina. No fetal tissue is seen. A blood specimen is sent for quantitative β-hCG level and an ultrasound is performed. A viable fetus is noted with a normal heart rate. The obstetrician sends her home with instructions to rest and avoid any physical activity, including sexual intercourse. She is also instructed to return to the emergency department if the bleeding is excessive. Which of the following did the patient experience today?
A 32-year-old woman presents to the emergency department with abdominal pain. She states it started last night and has been getting worse during this time frame. She states she is otherwise healthy and does not use drugs. Her temperature is 99.0°F (37.2°C), blood pressure is 120/83 mmHg, pulse is 85/min, respirations are 12/min, and oxygen saturation is 98% on room air. A rectal exam is performed and the patient is subsequently disimpacted. Five kilograms of stool are removed from the patient and she subsequently states her symptoms have resolved. Initial laboratory tests are ordered as seen below. Urine: Color: Yellow Protein: Negative Red blood cells: Negative hCG: Positive A serum hCG is 1,000 mIU/mL. A transvaginal ultrasound does not demonstrate a gestational sac within the uterus. Which of the following is the best next step in management?
A 38-year-old woman presents to the emergency department with painless vaginal bleeding of sudden onset approx. 1 hour ago. The woman informs the doctor that, currently, she is in the 13th week of pregnancy. She also mentions that she was diagnosed with hyperemesis gravidarum during the 6th week of pregnancy. On physical examination, her temperature is 37.2°C (99.0°F), pulse rate is 110/min, blood pressure is 108/76 mm Hg, and respiratory rate is 20/min. A general examination reveals pallor. Examination of the abdomen suggests that the enlargement of the uterus is greater than expected at 13 weeks of gestation. An ultrasonogram shows the absence of a fetus and the presence of an intrauterine mass with multiple cystic spaces that resembles a bunch of grapes. The patient is admitted to the hospital and her uterine contents are surgically removed. The atypical tissue is sent for genetic analysis, which of the following karyotypes is most likely to be found?
A 29-year-old African-American woman, gravida 4, para 0, comes to the physician for evaluation of recurrent abortions. Each pregnancy resulted in spontaneous abortion in the second trimester. The patient has a history of joint pain, chronic migraines, and recurrent poorly defined, macular skin rashes. She also reports episodes in which her fingers become pale and cold, and then redden. She is sexually active with her husband and does not use contraceptives. The patient works as a landscape architect. Her mother has a history of endometriosis. The patient takes a daily prenatal multivitamin and occasionally sumatriptan. She appears tired. Temperature is 36.5°C (97.7°F), pulse is 65/min, and blood pressure is 110/65 mm Hg. Examination of the hands shows two ulcerations on the tip of the right index finger and multiple tiny hemorrhages under the nails. There is a purple reticular rash on both calves. Which of the following is most likely to confirm the diagnosis?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app