
High-risk pregnancies — MCQs

On this page
A 27-year-old woman, gravida 2, para 1, at 26 weeks' gestation comes to the emergency department because of vaginal bleeding and epistaxis for the past 2 days. She missed her last prenatal visit 2 weeks ago. Physical examination shows blood in the posterior pharynx and a uterus consistent in size with 23 weeks' gestation. Her hemoglobin concentration is 7.2 g/dL. Ultrasonography shows an intrauterine pregnancy with a small retroplacental hematoma and absent fetal cardiac activity. Further evaluation is most likely to show which of the following findings?
A 38-year-old woman, gravida 2, para 1, at 35 weeks' gestation comes to the emergency department because of an episode of vaginal bleeding that morning. The bleeding has subsided. She has had no prenatal care. Her previous child was delivered with a caesarean section because of a breech presentation. Her temperature is 37.1°C (98.8°F), pulse is 88/min, respirations are 14/min, and blood pressure is 125/85 mm Hg. The abdomen is nontender and the size of the uterus is consistent with a 35-week gestation. No contractions are felt. The fetal heart rate is 145/min. Her hemoglobin concentration is 12 g/dL, leukocyte count is 13,000/mm3, and platelet count is 350,000/mm3. Transvaginal ultrasound shows that the placenta covers the internal os. Which of the following is the most appropriate next step in management?
A 42-year-old G1P0 woman presents to an obstetrician for her first prenatal visit. She has been pregnant for about 10 weeks and is concerned about how pregnancy will affect her health. Specifically, she is afraid that her complicated medical history will be adversely affected by her pregnancy. Her past medical history is significant for mild polycythemia, obesity hypoventilation syndrome, easy bleeding, multiple sclerosis, and aortic regurgitation. Which of these disorders is most likely to increase in severity during the course of the pregnancy?
A 31-year-old G3P2 who is at 24 weeks gestation presents for a regular check-up. She has no complaints, no concurrent diseases, and her previous pregnancies were vaginal deliveries with birth weights of 3100 g and 4180 g. The patient weighs 78 kg (172 lb) and is 164 cm (5 ft 5 in) in height. She has gained 10 kg (22 lb) during the current pregnancy. Her vital signs and physical examination are normal. The plasma glucose level is 190 mg/dL after a 75-g oral glucose load. Which of the listed factors contributes to the pathogenesis of the patient’s condition?
An otherwise healthy 25-year-old primigravid woman at 31 weeks' gestation comes to the physician with a 2-day history of epigastric pain and nausea that is worse at night. Three years ago, she was diagnosed with a peptic ulcer and was treated with a proton pump inhibitor and antibiotics. Medications include folic acid and a multivitamin. Her pulse is 92/min and blood pressure is 139/90 mm Hg. Pelvic examination shows a uterus consistent in size with a 31-week gestation. Laboratory studies show: Hemoglobin 8.2 g/dL Platelet count 87,000/mm3 Serum Total bilirubin 1.4 mg/dL Aspartate aminotransferase 75 U/L Lactate dehydrogenase 720 U/L Urine pH 6.1 Protein 2+ WBC negative Bacteria occasional Nitrites negative Which of the following best explains this patient's symptoms?
A 28-year-old woman, gravida 2, para 1, at 30 weeks' gestation comes to the physician because of headache for the past 5 days. Her pregnancy has been uncomplicated to date. Pregnancy and vaginal delivery of her first child were uncomplicated. The patient does not smoke or drink alcohol. She does not use illicit drugs. Medications include folic acid and a multivitamin. Her temperature is 37°C (98.6°F), pulse is 82/min, and blood pressure is 150/92 mm Hg. Physical examination reveals 2+ pitting edema in the lower extremities. Laboratory studies show: Hemoglobin 11.8 g/dL Platelet count 290,000/mm3 Urine pH 6.3 Protein 2+ WBC negative Bacteria occasional Nitrites negative The patient is at increased risk of developing which of the following complications?
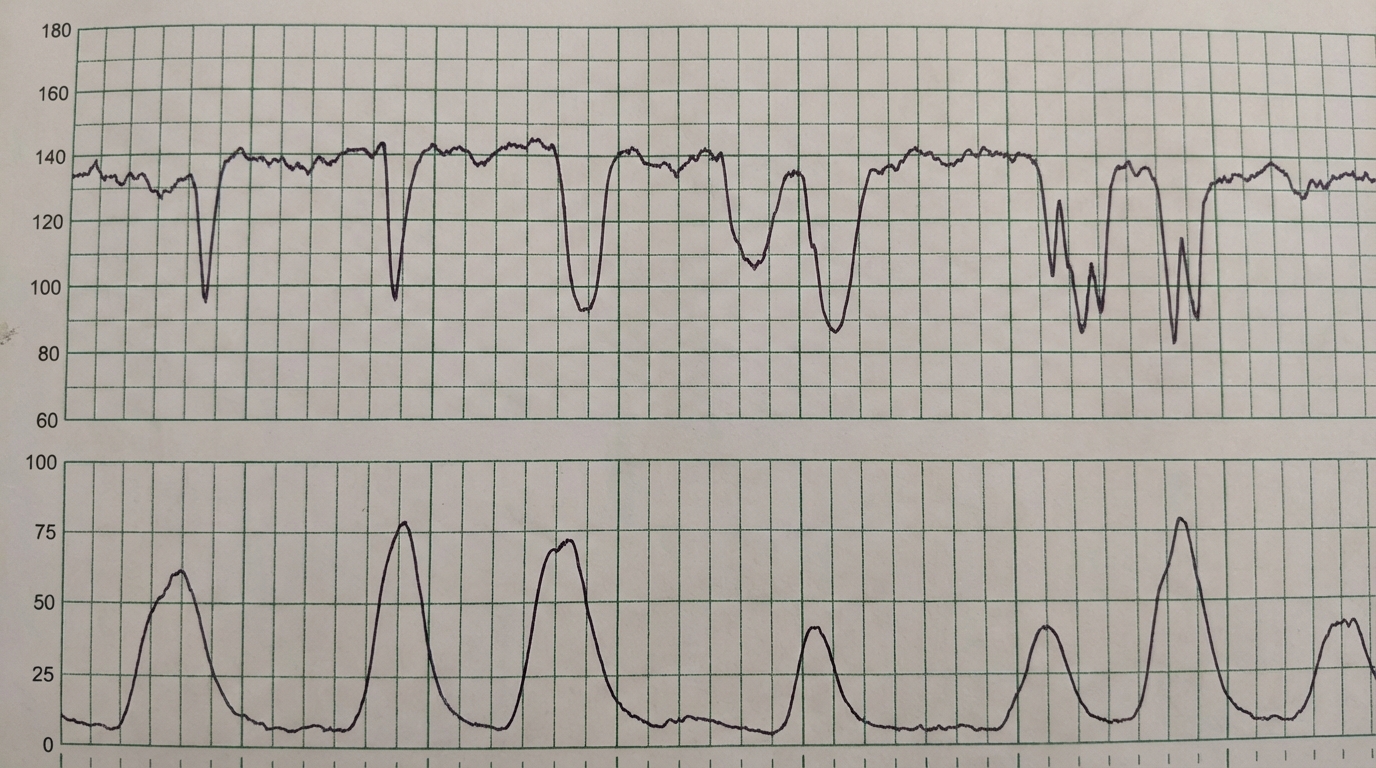
A 37-year-old primigravid woman at 36 weeks' gestation is admitted to the hospital 30 minutes after the onset of labor. On arrival, contractions occur every 8–10 minutes. During the last 2 days she has noted decreased fetal movements. The pregnancy had been complicated by gestational hypertension. Current medications include labetalol and a pregnancy multivitamin. Her temperature is 36.8°C (98.2°F), pulse is 94/min, and blood pressure is 154/96 mm Hg. On pelvic examination, the cervix is 40% effaced and 2 cm dilated; the vertex is at -2 station. The uterus is consistent in size with a 30-week gestation. Ultrasonography shows the fetus in vertex position and a decreased amount of amniotic fluid. A fetal heart tracing is shown. Which of the following is the most likely mechanism causing the variable decelerations seen on the fetal heart tracing?
A 25-year-old woman comes to the emergency department one hour after the sudden onset of diffuse abdominal pain and nausea. She has no history of serious illness. Menses occur at regular 27-day intervals and last 4 to 6 days with moderate flow. Her last menstrual period was 6 weeks ago. She is sexually active with two sexual partners and uses oral contraceptive pills inconsistently. She appears pale and diaphoretic. Her temperature is 37.7°C (99.9°F), pulse is 120/min, respirations are 20/min, and blood pressure is 85/70 mm Hg. Abdominal examination shows diffuse abdominal tenderness. Pelvic examination shows a normal appearing vagina, cervix, and uterus, with right adnexal tenderness. Her hemoglobin concentration is 13 g/dL, leukocyte count is 10,000/mm3, and platelet count is 350,000/mm3. Results of a pregnancy test are pending. Which of the following is the most appropriate next step in management?
A 27-year-old G2P0A2 woman comes to the office complaining of light vaginal spotting. She received a suction curettage 2 weeks ago for an empty gestational sac. Pathology reports showed hyperplastic and hydropic trophoblastic villi, but no fetal tissue. The patient denies fever, abdominal pain, dysuria, dyspareunia, or abnormal vaginal discharge. She has no chronic medical conditions. Her periods are normally regular and last 3-4 days. One year ago, she had an ectopic pregnancy that was treated with methotrexate. She has a history of chlamydia and gonorrhea that was treated 5 years ago with azithromycin and ceftriaxone. Her temperature is 98°F (36.7°C), blood pressure is 125/71 mmHg, and pulse is 82/min. On examination, hair is present on the upper lip, chin, and forearms. A pelvic examination reveals a non-tender, 6-week-sized uterus and bilateral adnexal masses. There is scant dark blood in the vaginal vault on speculum exam. A quantitative beta-hCG is 101,005 mIU/mL. Two weeks ago, her beta-hCG was 63,200 mIU/mL. A pelvic ultrasound shows bilaterally enlarged ovaries with multiple thin-walled cysts between 2-3 cm in size. Which of the following is the most likely cause of the patient’s adnexal masses?
A 36-year-old woman comes to the physician because she has not had her menstrual period for the past 4 months. During this period, she has had frequent headaches, difficulty sleeping, and increased sweating. She has not had any weight changes. Over the past year, menses occurred at irregular 30- to 45-day intervals with light flow. The patient underwent two successful cesarean sections at the ages of 28 and 32. She has two healthy children. She is sexually active with her husband and does not use condoms. Her vital signs are within normal limits. Physical examination shows no abnormalities. Laboratory studies show: Estradiol 8 pg/mL (mid-follicular phase: N=27–123 pg/mL) Follicle-stimulating hormone 200 mIU/mL Luteinizing hormone 180 mIU/mL Prolactin 16 ng/mL Which of the following is the most likely diagnosis?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app