
High-risk pregnancies — MCQs

On this page
A 36-year-old African American G1P0010 presents to her gynecologist for an annual visit. She has a medical history of hypertension, for which she takes hydrochlorothiazide. The patient’s mother had breast cancer at age 68, and her sister has endometriosis. At this visit, the patient’s temperature is 98.6°F (37.0°C), blood pressure is 138/74 mmHg, pulse is 80/min, and respirations are 13/min. Her BMI is 32.4 kg/m^2. Pelvic exam reveals a nontender, 16-week sized uterus with an irregular contour. A transvaginal ultrasound is performed and demonstrates a submucosal leiomyoma. This patient is at most increased risk of which of the following complications?
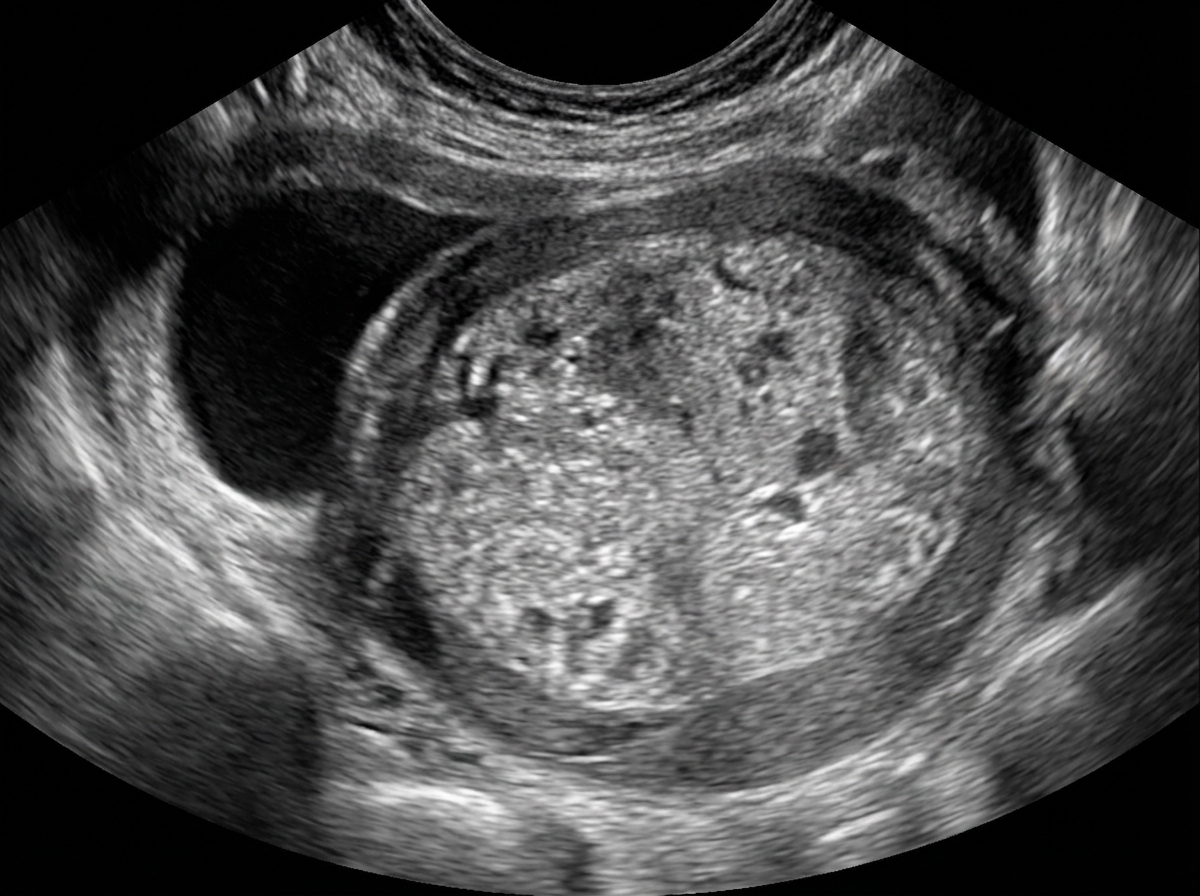
A 28-year-old primigravid woman comes to the emergency department because of a 12-hour history of lower abdominal pain and vaginal bleeding. She also had nausea and fatigue for the past 3 weeks. Her last menstrual period was 8 weeks ago. Prior to that, her menses occurred regularly at 30-day intervals and lasted for 4 days. There is no history of medical illness, and she takes no medications. Her temperature is 37°C (98.6°F), pulse is 95/min, and blood pressure is 100/70 mm Hg. Pelvic examination is painful and shows a uterus consistent in size with a 13-week gestation. A urine pregnancy test is positive. β-HCG level is 106,000 mIU/mL (N < 5 mIU/mL). Transvaginal ultrasonography shows unclear, amorphous fetal parts and a large placenta with multiple cystic spaces. Which of the following is the most likely cause of this patient's condition?
A 44-year-old G2P2 African American woman presents to her gynecologist for dysmenorrhea. She reports that for the past few months, she has been having severe pain during her menses. She also endorses menstrual bleeding that has been heavier than usual. The patient reports that her cycles are regular and occur every 30 days, and she denies both dyspareunia and spotting between her periods. Her last menstrual period was two weeks ago. In terms of her obstetric history, the patient had two uncomplicated pregnancies, and she had no difficulty becoming pregnant. She has never had an abnormal pap smear. Her past medical history is otherwise significant for hyperlipidemia and asthma. On physical exam, the patient’s uterus is tender, soft, and enlarged to the size of a pregnant uterus at 10 weeks of gestation. She is non-tender during vaginal exam, without cervical motion tenderness or adnexal masses. Her BMI is 24 kg/m2. A urine pregnancy test is negative. Which of the following is the most likely diagnosis for this patient?
A 36-year-old primigravid woman comes to the physician for a prenatal visit at 14 weeks' gestation. She has had episodic headaches over the past month. At home, blood pressure measurements have ranged from 134/82 mm Hg to 148/94 mm Hg. Today, her blood pressure is 146/91 mm Hg. Pelvic examination shows a uterus consistent in size with a 13-week gestation. Serum creatinine is 0.8 mg/dL, serum ALT is 17 U/L, and platelet count is 320,000/mm3. Urinalysis shows no abnormalities. Which of the following is the most likely diagnosis?
A 52-year-old woman comes to the physician because of vaginal itchiness and urinary frequency for the past 1 year. She stopped having vaginal intercourse with her husband because it became painful and occasionally resulted in vaginal spotting. Her last menstrual cycle was 14 months ago. She has vitiligo. Her only medication is a topical tacrolimus ointment. Her temperature is 37.1°C (98.8°F), pulse is 85/min, and blood pressure is 135/82 mm Hg. Examination shows multiple white maculae on her forearms, abdomen, and feet. Pelvic examination shows scarce pubic hair, vulvar pallor, and narrowing of the vaginal introitus. Which of the following most likely contributes to this patient's current symptoms?
A 62-year-old woman makes an appointment with her primary care physician because she recently started experiencing post-menopausal bleeding. She states that she suffered from anorexia as a young adult and has been thin throughout her life. She says that this nutritional deficit is likely what caused her to not experience menarche until age 15. She used oral contraceptive pills for many years, has never been pregnant, and experienced menopause at age 50. A biopsy of tissue inside the uterus reveals foci of both benign and malignant glandular cells. Which of the following was a risk factor for the development of the most likely cause of her symptoms?
A 52-year-old woman presents to her gynecologist's office with complaints of frequent hot flashes and significant sweating episodes, which affect her sleep at night. She complains that she has to change her clothes in the middle of the night because of the sweating events. She also complains of irritability, which is affecting her relationships with her husband and daughter. She reports vaginal itchiness and pain with intercourse. Her last menstrual period was eight months ago. She was diagnosed with breast cancer 15 years ago, which was promptly detected and cured successfully via mastectomy. The patient is currently interested in therapies to help control her symptoms. Which of the following options is the most appropriate HORMONAL therapy in this patient for her genitourinary symptoms?
A 32-year-old G2P1 female at 30 weeks gestation presents to the emergency department with complaints of vaginal bleeding and severe abdominal pain. She states that she began feeling poorly yesterday with a stomach-ache, nausea, and vomiting. She first noted a small amount of spotting this morning that progressed to much larger amounts of vaginal bleeding with worsened abdominal pain a few hours later, prompting her to come to the emergency department. Her previous pregnancy was without complications, and the fetus was delivered at 40 weeks by Cesarean section. Fetal heart monitoring shows fetal distress with late decelerations. Which of the following is a risk factor for this patient's presenting condition?
A 16-year-old girl is brought to the physician because she has not attained menarche. There is no personal or family history of serious illness. She is 165 cm (5 ft 5 in) tall and weighs 60 kg (132 lb); BMI is 22 kg/m2. Breast development is Tanner stage 4, and pubic hair development is Tanner stage 1. Pelvic examination shows a blind vaginal pouch. This patient is most likely to have which of the following karyotypes?
A 17-year-old girl is brought to the physician because of amenorrhea for 4 months. Menses previously occurred at regular 28-day intervals and last for 3 to 4 days. There is no family history of serious illness. She receives good grades in school and is on the high school track team. She is sexually active with one male partner and uses condoms consistently. She appears thin. Examination shows bilateral parotid gland enlargement. There is fine hair over the trunk. Serum studies show: Thyroid-stimulating hormone 3.7 μU/mL Prolactin 16 ng/mL Estradiol 23 pg/mL (N > 40) Follicle-stimulating hormone 1.6 mIU/mL Luteinizing hormone 2.8 mIU/mL A urine pregnancy test is negative. Which of the following is the most likely cause of these findings?
Practice by Chapter
Advanced maternal age
Practice Questions
Multiple gestation management
Practice Questions
Pregestational diabetes
Practice Questions
Chronic hypertension in pregnancy
Practice Questions
Thyroid disorders in pregnancy
Practice Questions
Autoimmune disorders in pregnancy
Practice Questions
Cardiac disease in pregnancy
Practice Questions
Renal disease in pregnancy
Practice Questions
Obesity in pregnancy
Practice Questions
Substance use in pregnancy
Practice Questions
Prior preterm birth management
Practice Questions
Prior cesarean delivery management
Practice Questions
Maternal cancer in pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app