
Protozoa/Helminths — MCQs

On this page
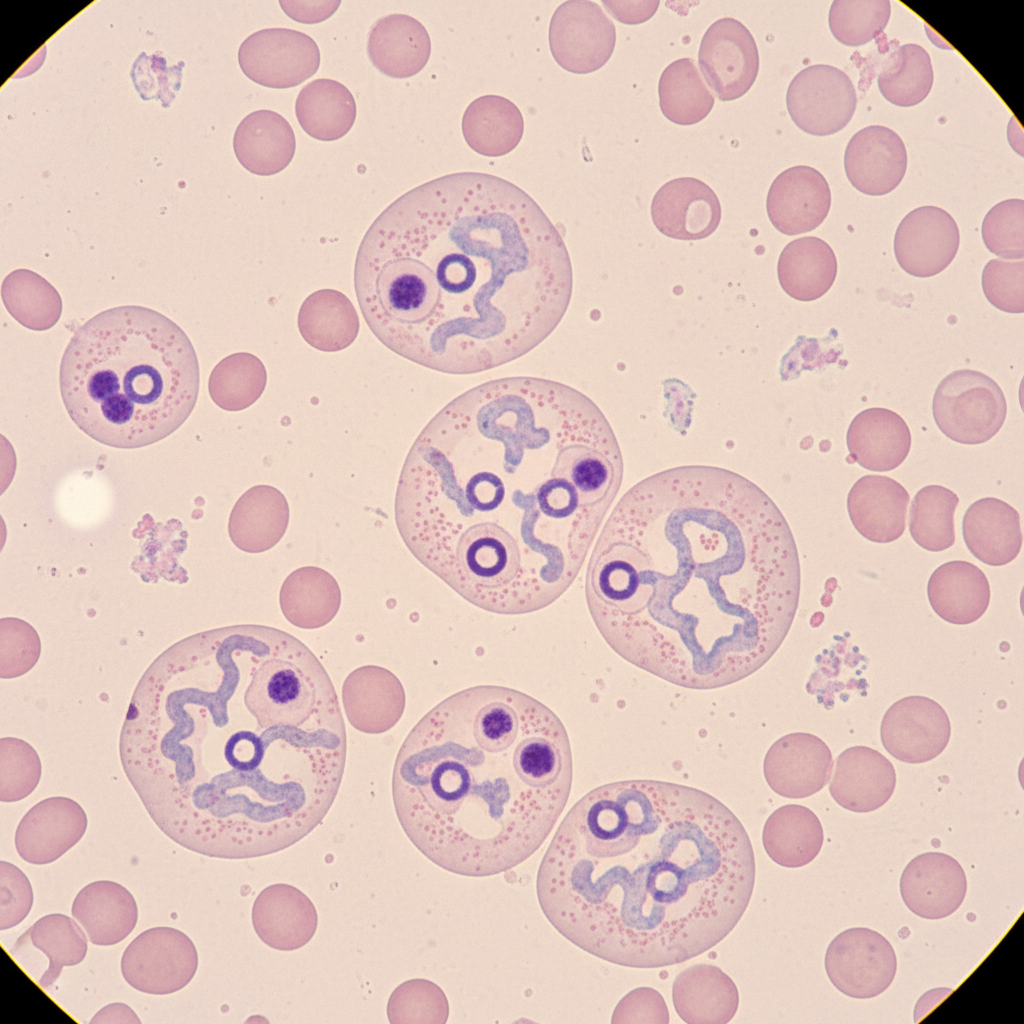
A 42-year-old man presents with unremitting diarrhea that has lasted for 2 weeks. He describes his bowel movements as watery, non-bloody, foul-smelling, and greasy. He also has cramping abdominal pain associated with the diarrhea. He says that his symptoms started right after he returned from a father-son camping trip to the mountains. His son has similar symptoms. His vital signs include: pulse 78/min, respiratory rate 15/min, temperature 37.2°C (99.0°F), and blood pressure 120/70 mm Hg. A stool sample is obtained and microscopic analysis is significant for the findings shown in the image below. Which of the following pathogens is most likely responsible for this patient’s condition?

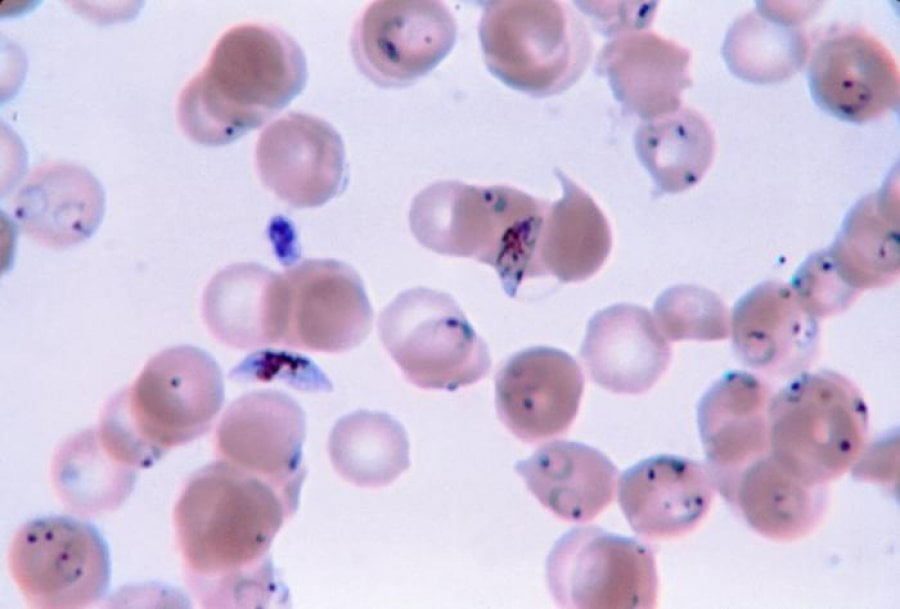
A 55-year-old woman comes to the physician because of fever, chills, headache, and nausea over the past 3 days. Nine months ago, she returned from a vacation in Indonesia where she had experienced similar symptoms and episodic fever. She was treated with chloroquine and recovered uneventfully. Her temperature is 39.1°C (102.4°F), pulse is 97/min, and blood pressure is 123/85 mm Hg. Physical examination shows scleral icterus. The abdomen is soft; bowel sounds are active. Neurologic examination is unremarkable. Her hemoglobin concentration is 10 g/dL. A photomicrograph of a peripheral blood smear is shown. Which of the following is the most likely cause of the recurrence of symptoms in this patient?
A 27-year-old previously healthy man presents to the clinic complaining of bloody diarrhea and abdominal pain. Sexual history reveals that he has sex with men and women and uses protection most of the time. He is febrile with all other vital signs within normal limits. Physical exam demonstrates tenderness to palpation of the right upper quadrant. Subsequent ultrasound shows a uniform cyst in the liver. In addition to draining the potential abscess and sending it for culture, appropriate medical therapy would involve which of the following?
A 37-year-old man makes an appointment with his primary care physician because he has been feeling tired and is no longer able to play on a recreational soccer team. He also says his coworkers have commented that he appears pale though he has not noticed any changes himself. He says that he has been generally healthy and that the only notable event that happened in the last year is that he went backpacking all over the world. Based on clinical suspicion, a series of blood tests are performed with partial results presented below: Hemoglobin: 9.8 g/dL Platelet count: 174,000/mm^3 Mean corpuscular volume: 72 µm^3 (normal: 80-100 µm^3) Iron: 22 µg/dL (normal: 50-170 µg/dL) Ferritin: 8 ng/mL (normal: 15-200 ng/mL) Lactate dehydrogenase: 57 U/L (normal: 45-90 U/L) Urine hemoglobin: absent Infection with which of the following types of organisms could lead to this pattern of findings?
A 46-year-old man comes to the physician because of a 1-week history of headache, muscle pain, and recurrent fever spikes that occur without a noticeable rhythm. Two weeks ago, he returned from a 5-week-long world trip during which he climbed several mountains in India, Africa, and Appalachia. Chemoprophylaxis with chloroquine was initiated one week prior to the trip. Physical examination shows jaundice. The spleen is palpated 2 cm below the left costal margin. His hemoglobin concentration is 10 g/dL. A photomicrograph of a peripheral blood smear is shown. Which of the following agents is the most likely cause of this patient's findings?
A 41-year-old male with a history of Pneumocystis jirovecii pneumonia is found to have multiple ring-enhancing lesions on brain CT. Which of the following is most likely responsible for this patient's abnormal scan?
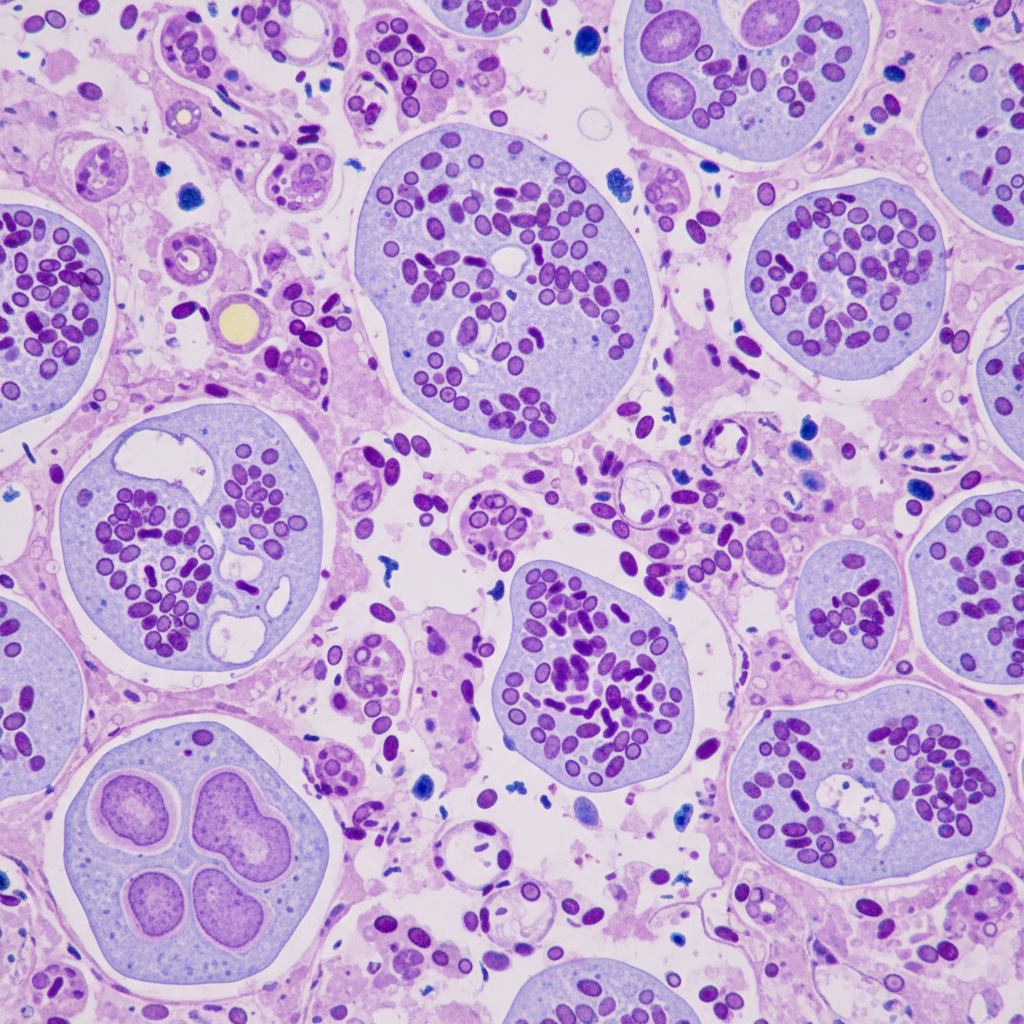
A 34-year-old man comes to the physician for a 2-month history of an itchy rash on his forearm. He feels well otherwise and has not had any fever or chills. He returned from an archaeological expedition to Guatemala 4 months ago. Skin examination shows a solitary, round, pink-colored plaque with central ulceration on the right wrist. There is right axillary lymphadenopathy. A photomicrograph of a biopsy specimen from the lesion is shown. Which of the following is the most likely causal organism?
Practice by Chapter
Malaria parasites and life cycle
Practice Questions
Intestinal protozoa (Giardia, Entamoeba)
Practice Questions
Toxoplasma gondii
Practice Questions
Trypanosomes
Practice Questions
Leishmania species
Practice Questions
Nematodes (roundworms)
Practice Questions
Cestodes (tapeworms)
Practice Questions
Trematodes (flukes)
Practice Questions
Blood and tissue parasites
Practice Questions
Antiparasitic medications
Practice Questions
Laboratory diagnosis of parasites
Practice Questions
Global health impact of parasitic infections
Practice Questions
Ectoparasites and vector-borne diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app