
Intestinal protozoa (Giardia, Entamoeba) — MCQs

A 27-year-old male who works on an organic farm is diagnosed with infection by N. americanus, a helminthic parasite. Eosinophils require which antibody isotype to destroy these parasites via antibody-dependent cellular cytotoxicity?
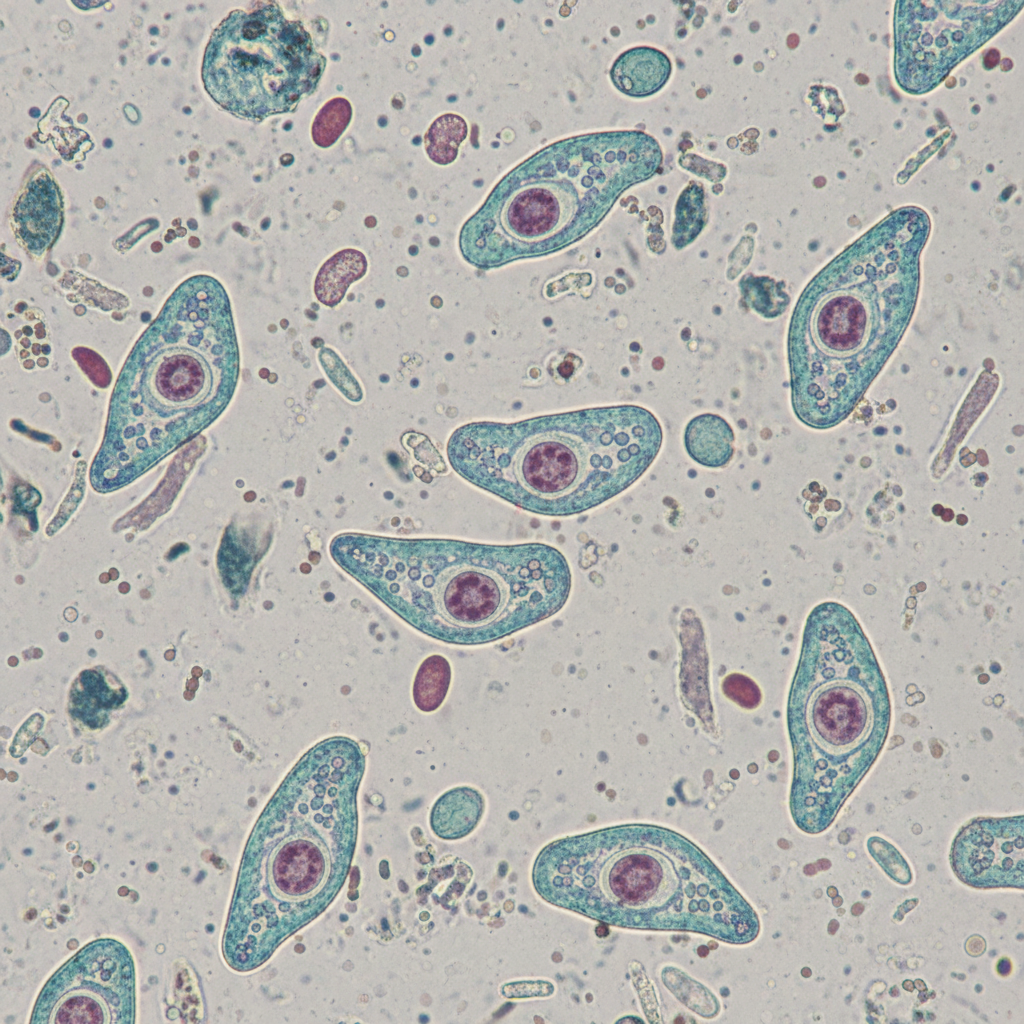
A 29-year-old man presents to the clinic with several days of flatulence and greasy, foul-smelling diarrhea. He says that he was on a camping trip last week after which his symptoms started. When asked further about his camping activities, he reports collecting water from a stream but did not boil or chemically treat the water. The patient also reports nausea, weight loss, and abdominal cramps followed by sudden diarrhea. He denies tenesmus, urgency, and bloody diarrhea. His temperature is 37°C (98.6° F), respiratory rate is 15/min, pulse is 107/min, and blood pressure is 89/58 mm Hg. A physical examination is performed where nothing significant was found except for dry mucous membranes. Intravenous fluids are started and a stool sample is sent to the lab, which reveals motile protozoa on microscopy, negative for any ova, no blood cells, and pus cells. What is the most likely diagnosis?
A 34-year-old woman with HIV comes to the emergency department because of a 2-week history of diarrhea and abdominal cramping. She has had up to 10 watery stools per day. She also has anorexia and nausea. She returned from a trip to Mexico 4 weeks ago where she went on two hiking trips and often drank from spring water. She was diagnosed with HIV 12 years ago. She says that she has been noncompliant with her therapy. Her last CD4+ T-lymphocyte count was 85/mm3. She appears thin. She is 175 cm (5 ft 9 in) tall and weighs 50 kg (110 lb); BMI is 16.3 kg/m2. Her temperature is 38.3°C (100.9°F), pulse is 115/min, and blood pressure is 85/65 mm Hg. Examination shows dry mucous membranes. The abdomen is soft, and there is diffuse tenderness to palpation with no guarding or rebound. Bowel sounds are hyperactive. Microscopy of a modified acid-fast stain on a stool sample reveals oocysts. Which of the following is the most likely causal organism?
A 31-year-old man comes to the physician because of a 2-day history of abdominal pain and diarrhea. He reports that his stools are streaked with blood and mucus. He returned from a vacation in the Philippines 3 weeks ago. His vital signs are within normal limits. Abdominal examination shows hyperactive bowel sounds. A photomicrograph of a trichrome-stained wet mount of a stool specimen is shown. Which of the following organisms is the most likely cause of this patient's symptoms?
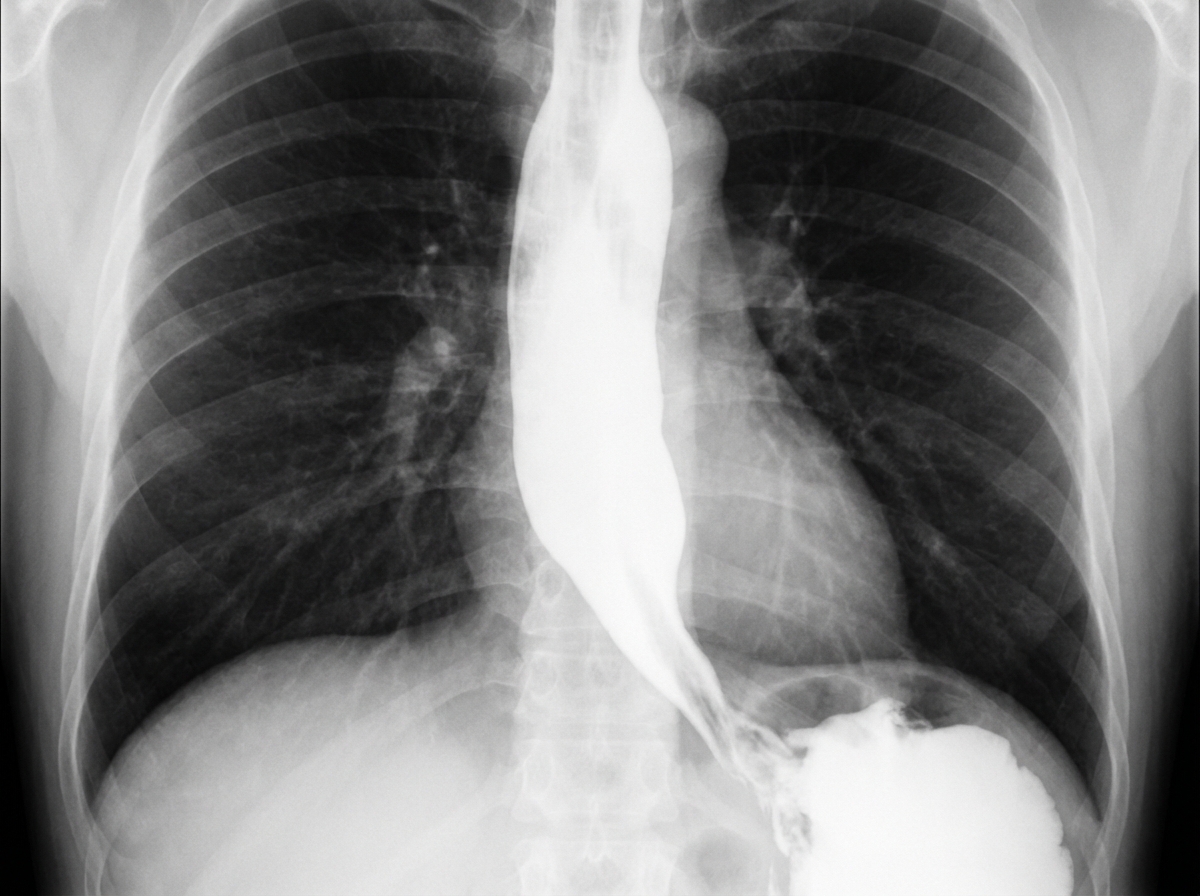
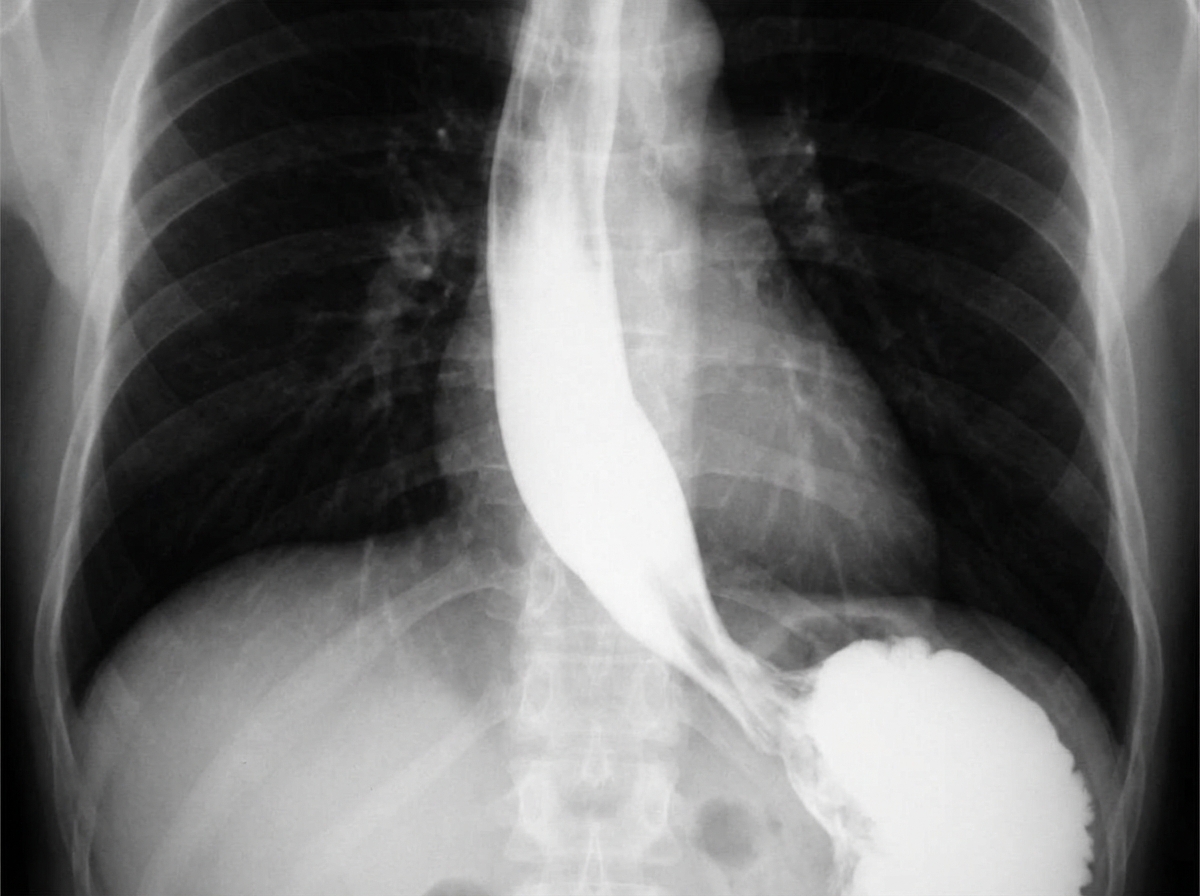
A 62-year-old man is referred to a gastroenterologist because of difficulty swallowing for the past 5 months. He has difficulty swallowing both solid and liquid foods, but there is no associated pain. He denies any shortness of breath or swelling in his legs. He immigrated from South America 10 years ago. He is a non-smoker and does not drink alcohol. His physical examination is unremarkable. A barium swallow study was ordered and the result is given below. Esophageal manometry confirms the diagnosis. What is the most likely underlying cause of this patient’s condition?
A 48-year-old man presents to the clinic with several weeks of watery diarrhea and right upper quadrant pain with fever. He also endorses malaise, nausea, and anorexia. He is HIV-positive and is currently on antiretroviral therapy. He admits to not being compliant with his current medications. His temperature is 37°C (98.6°F), respiratory rate is 15/min, pulse is 70/min, and blood pressure is 100/84 mm Hg. A physical examination is performed which is within normal limits. His blood tests results are given below: Hb%: 11 gm/dL Total count (WBC): 3,400 /mm3 Differential count: Neutrophils: 70% Lymphocytes: 25% Monocytes: 5% CD4+ cell count: 88/mm3 Stool microscopy results are pending. What is the most likely diagnosis?
A 48-year-old man from Argentina presents to your office complaining of difficulty swallowing for the past few months. He is accompanied by his wife who adds that his breath has started to smell horrible. The patient says that he feels uncomfortable no matter what he eats or drinks. He also has lost 5 kg (11 lb) in the last 2 months. The patient is afebrile, and his vital signs are within normal limits. Physical exam is unremarkable. A barium swallow study along with esophageal manometry is performed and the results are shown in the image below. Manometry shows very high pressure at the lower esophageal sphincter. Which of the following is the most likely etiology of this patient’s symptoms?
A 36-year-old man is brought to the emergency department for right upper quadrant abdominal pain that began 3 days ago. The pain is nonradiating and has no alleviating or exacerbating factors. He denies any nausea or vomiting. He immigrated from Mexico 6 months ago and currently works at a pet shop. He has been healthy except for 1 week of bloody diarrhea 5 months ago. He is 182 cm (5 ft 11 in) tall and weighs 120 kg (264 lb); BMI is 36 kg/m2. His temperature is 101.8°F (38.8°C), pulse is 85/min, respirations are 14/min, and blood pressure is 120/75 mm Hg. Lungs are clear to auscultation. He has tenderness to palpation in the right upper quadrant. Laboratory studies show: Hemoglobin 11.7 g/dL3 Leukocyte Count 14,000/mm Segmented neutrophils 74% Eosinophils 2% Lymphocytes 17% Monocytes 7% Platelet count 140,000/mm3 Serum Na+ 139 mEq/L Cl- 101 mEq/L K+ 4.4 mEq/L HCO3- 25 mEq/L Urea nitrogen 8 mg/dL Creatinine 1.6 mg/dL Total bilirubin 0.4 mg/dL AST 76 U/L ALT 80 U/L Alkaline phosphatase 103 U/L Ultrasonography of the abdomen shows a 4-cm round, hypoechoic lesion in the right lobe of the liver with low-level internal echoes. Which of the following is the most likely diagnosis?
A 26-year-old woman comes to the physician because of several days of fever, abdominal cramps, and diarrhea. She drank water from a stream 1 week ago while she was hiking in the woods. Abdominal examination shows increased bowel sounds. Stool analysis for ova and parasites shows flagellated multinucleated trophozoites. Further evaluation shows the presence of antibodies directed against the pathogen. Secretion of these antibodies most likely requires binding of which of the following?
A 30-year-old Caucasian male is brought to the emergency room for recurrent diarrhea. He has had multiple upper respiratory infections since birth and does not take any medications at home. It is determined that Giardia lamblia is responsible for the recurrent diarrhea. The physician performs a serum analysis and finds normal levels of mature B lymphocytes. What other finding on serum analysis predisposes the patient to recurrent diarrheal infections?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app