
Parasitic life cycles — MCQs

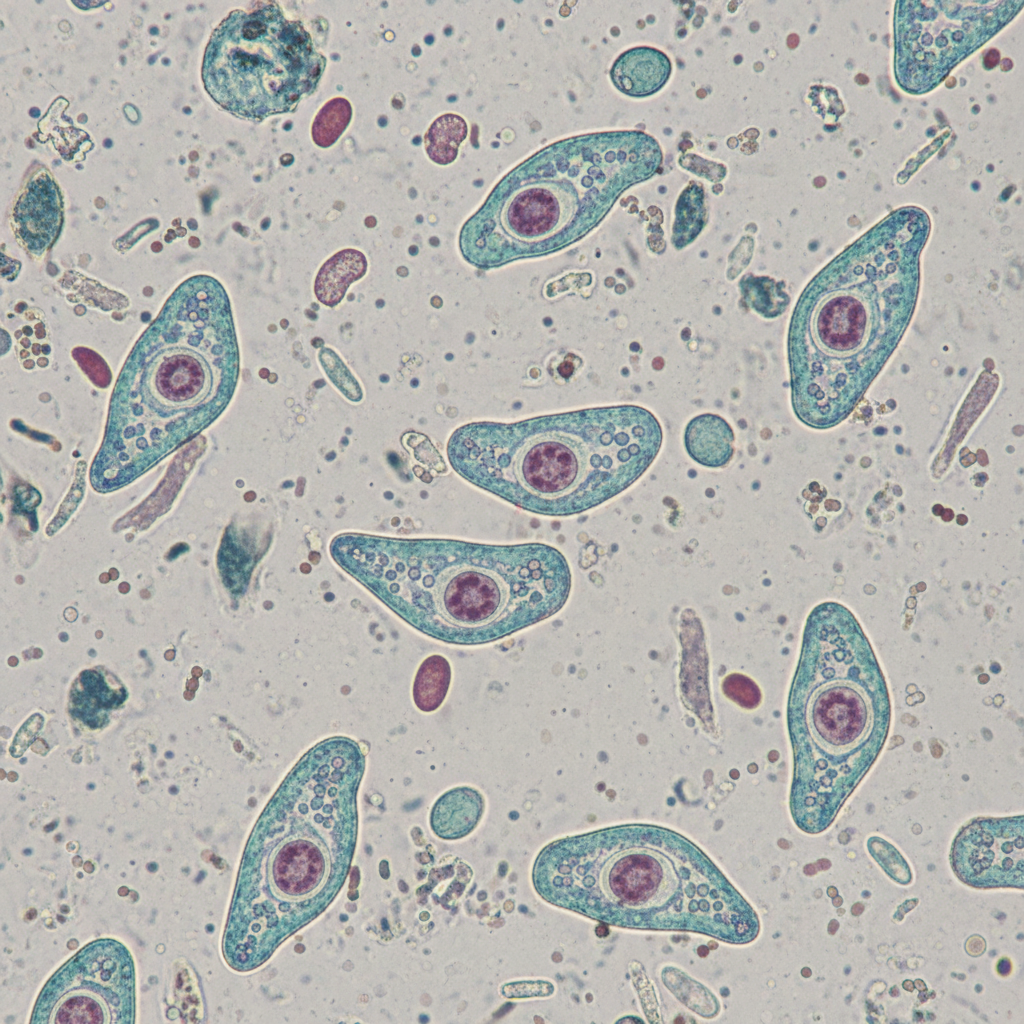
A 31-year-old man comes to the physician because of a 2-day history of abdominal pain and diarrhea. He reports that his stools are streaked with blood and mucus. He returned from a vacation in the Philippines 3 weeks ago. His vital signs are within normal limits. Abdominal examination shows hyperactive bowel sounds. A photomicrograph of a trichrome-stained wet mount of a stool specimen is shown. Which of the following organisms is the most likely cause of this patient's symptoms?
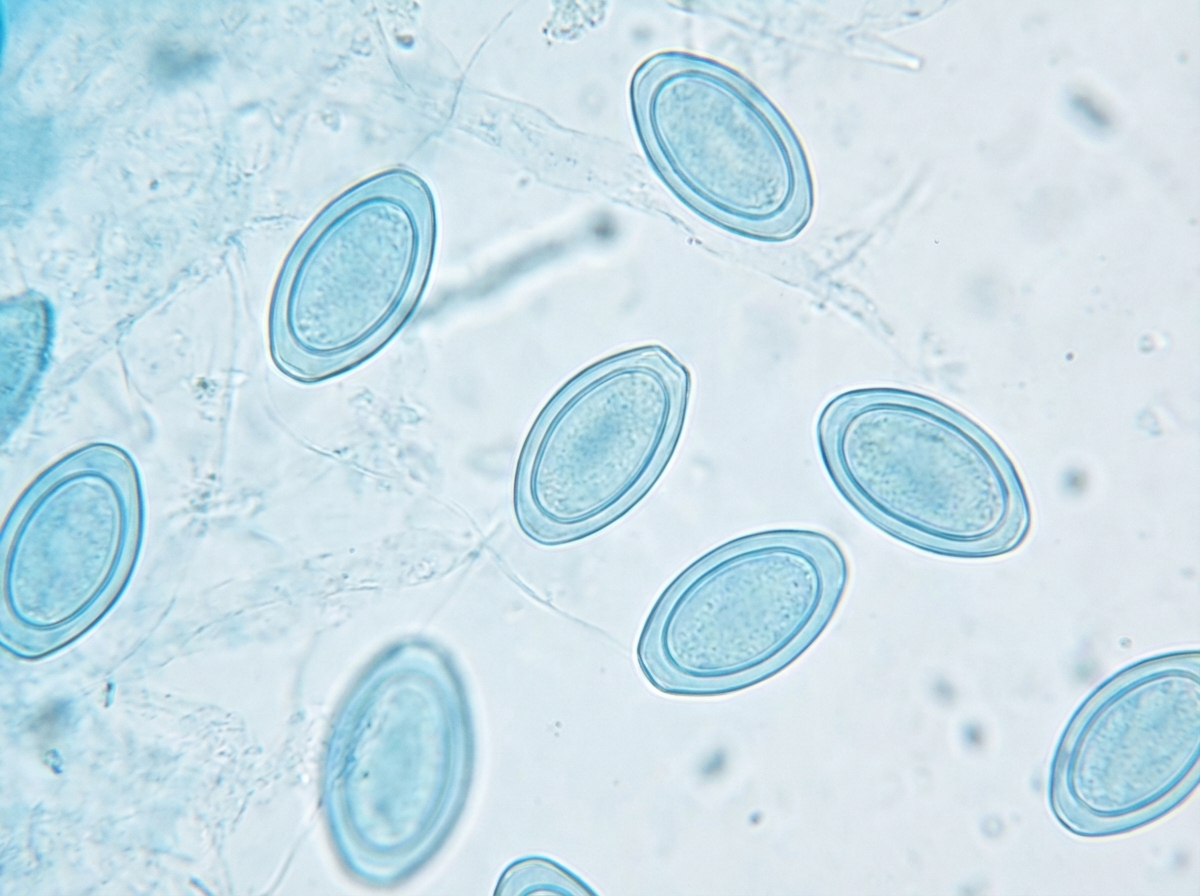
A 2-year-old girl is brought to the doctor by her mother with persistent scratching of her perianal region. The patient’s mother says that symptoms started 3 days ago and have progressively worsened until she is nearly continuously scratching even in public places. She says that the scratching is worse at night and disturbs her sleep. An anal swab and staining with lactophenol cotton blue reveal findings in the image (see image). Which of the following is the organism most likely responsible for this patient’s condition?
A 13-year-old boy is brought to a physician with severe fevers and headaches for 3 days. The pain is constant and mainly behind the eyes. He has myalgias, nausea, vomiting, and a rash for one day. Last week, during an academic winter break, he traveled on a tour with his family to several countries, including Brazil, Panama, and Peru. They spent many evenings outdoors without any protection against insect bites. There is no history of contact with pets, serious illness, or use of medications. The temperature is 40.0℃ (104.0℉); the pulse is 110/min; the respiratory rate is 18/min, and the blood pressure is 110/60 mm Hg. A maculopapular rash is seen over the trunk and extremities. Several tender lymph nodes are palpated in the neck on both sides. A peripheral blood smear shows no organisms. Which of the following is most likely responsible for this patient’s presentation?
A 32-year-old woman presents to your office with abdominal pain and bloating over the last month. She also complains of intermittent, copious, non-bloody diarrhea over the same time. Last month, she had a cough that has since improved but has not completely resolved. She has no sick contacts and has not left the country recently. She denies any myalgias, itching, or rashes. Physical and laboratory evaluations are unremarkable. Examination of her stool reveals the causative organism. This organism is most likely transmitted to the human host through which of the following routes?
A 31-year-old male traveler in Thailand experiences fever, headache, and excessive sweating every 48 hours. Peripheral blood smear shows trophozoites and schizonts indicative of Plasmodia infection. The patient is given chloroquine and primaquine. Primaquine targets which of the following Plasmodia forms:
A 52-year-old man presents with a 5-week history of multiple cutaneous ulcers on his left forearm and neck, which he first noticed after returning from a 2-month stay in rural Peru. He does not recall any trauma or arthropod bites. The lesions began as non-pruritic erythematous papules that became enlarged, ulcerated, and crusted. There is no history of fever or abdominal pain. He has been sexually active with a single partner since their marriage at 24 years of age. The physical examination reveals erythematous, crusted plaques with central ulceration and a raised border. There is no fluctuance, drainage, or sporotrichoid spread. A punch biopsy was performed, which revealed an ulcerated lesion with a mixed inflammatory infiltrate. Amastigotes within dermal macrophages are seen on Giemsa staining. What is the most likely diagnosis?
A 68-year-old man presents to his physician for symptoms of chronic weight loss, abdominal bloating, and loose stools. He notes that he has also been bothered by a chronic cough. The patient’s laboratory work-up includes a WBC differential, which is remarkable for an eosinophil count of 9%. Stool samples are obtained, with ova and parasite examination revealing roundworm larvae in the stool and no eggs. Which of the following parasitic worms is the cause of this patient’s condition?
A 30-year-old man presents to the physician after he discovered a raised, red, string-shaped lesion beneath the skin on his right foot. The lesion seems to move from one location to another over the dorsum of his foot from day to day. He says that the lesion is extremely itchy and has not responded to over the counter topical treatment. He and his wife recently returned from a honeymoon in southern Thailand, where they frequented the tropical beaches. The physician diagnoses him with a parasitic infection and prescribes albendazole for the patient. With which of the following organisms is the patient most likely infected?
A 31-year-old man comes to the physician because of severe muscle pain and fever for 4 days. He likes to go hunting and consumed bear meat 1 month ago. Examination shows periorbital edema and generalized muscle tenderness. His leukocyte count is 12,000/mm3 with 19% eosinophils. The release of major basic protein in response to this patient’s infection is most likely a result of which of the following?
A 38-year-old man comes to the physician because of a 2-week history of abdominal pain and an itchy rash on his buttocks. He also has fever, nausea, and diarrhea with mucoid stools. One week ago, the patient returned from Indonesia, where he went for vacation. Physical examination shows erythematous, serpiginous lesions located in the perianal region and the posterior thighs. His leukocyte count is 9,000/mm3 with 25% eosinophils. Further evaluation is most likely to show which of the following findings?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app