
Parasites/Fungi — MCQs

On this page
A 38-year-old man comes to the physician because of a 2-week history of abdominal pain and an itchy rash on his buttocks. He also has fever, nausea, and diarrhea with mucoid stools. One week ago, the patient returned from Indonesia, where he went for vacation. Physical examination shows erythematous, serpiginous lesions located in the perianal region and the posterior thighs. His leukocyte count is 9,000/mm3 with 25% eosinophils. Further evaluation is most likely to show which of the following findings?
A 28-year-old woman with a past history of type 1 diabetes presents to your office with a 2-week history of vaginal itching and soreness accompanied by a white, clumpy vaginal discharge which she says resembles cheese curds. Her last HbA1c from a month ago was 7.8%, and her last cervical cytology from 10 months ago was reported as normal. She has a blood pressure of 118/76 mmHg, respiratory rate of 14/min, and heart rate of 74/min. Pelvic examination reveals multiple small erythematous lesions in the inguinal and perineal area, vulvar erythema, and excoriations. Inspection demonstrates a normal cervix and a white, adherent, thick, non-malodorous vaginal discharge. Which of the following is most likely to be present in a saline wet mount from the vaginal discharge of this patient?
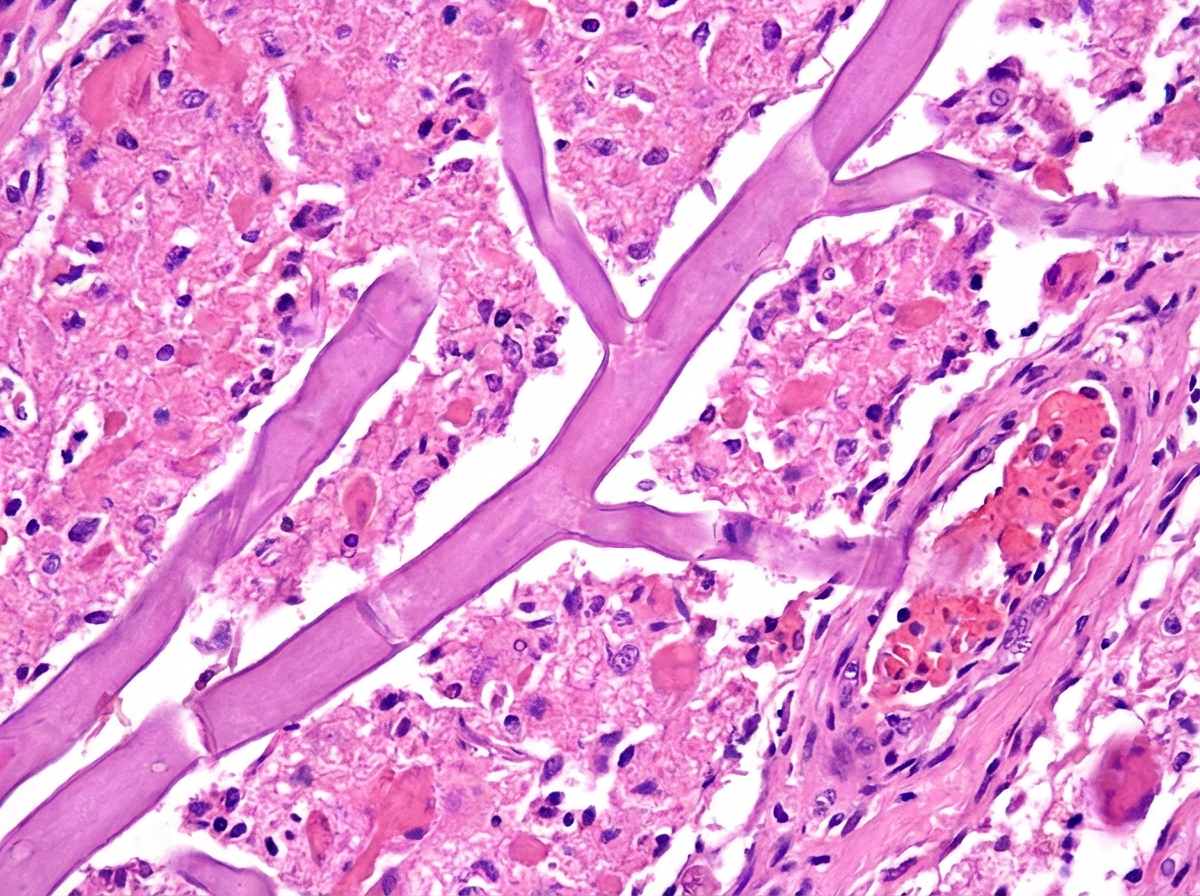
A 61-year-old man is brought to the emergency department by his wife because of increasing confusion over the past 12 hours. His wife reports that he has a history of type 1 diabetes mellitus. His temperature is 38.8°C (101.8°F). He is confused and oriented only to person. Examination shows left periorbital swelling that is tender to palpation, mucopurulent rhinorrhea, and a black necrotic spot over the nose. There is discharge of the left eye with associated proptosis. A photomicrograph of a specimen obtained on biopsy of the left maxillary sinus is shown. Which of the following is the most likely causal organism?
A 16-year-old boy is brought to the physician by his host parents for evaluation of a progressively pruritic rash over his shoulders and buttocks for the past 6 months. He recently came to the United States from Nigeria to attend a year of high school. He reports that it has been increasingly difficult for him to read the whiteboard during classes. Physical examination shows symmetrically distributed papules 4–8 mm in diameter, excoriation marks, and patchy hyperpigmentation over his shoulders, waist, and buttocks. There is nontender inguinal lymphadenopathy and several firm, nontender subcutaneous nodules along the right iliac crest. Six skin snip biopsies are taken from the pelvic girdle, buttocks, and thigh, and are then incubated in saline. After 24 hours, microscopic examination shows motile microfilariae. Which of the following is the most likely diagnosis?
A 67-year-old male presents to his primary care physician for evaluation of fever and an unintended weight loss of 25 pounds over the last 4 months. He also has decreased appetite and complains of abdominal pain located in the right upper quadrant. The patient has not noticed any changes in stool or urine. He emigrated from Malaysia to the United States one year prior. Social history reveals that he smokes half a pack per day and has 5-7 drinks of alcohol per day. The patient is up to date on all of his vaccinations. Physical exam findings include mild jaundice as well as an enlarged liver edge that is tender to palpation. Based on clinical suspicion, biomarker labs are sent and show polycythemia and an elevated alpha fetoprotein level but a normal CA 19-9 level. Surface antigen for hepatitis B is negative. Ultrasound reveals a normal sized gallbladder. Given this presentation, which of the following organisms was most likely associated with the development of disease in this patient?
A 45-year-old man presents to the emergency department with abdominal distension. The patient states he has had gradually worsening abdominal distension with undulating pain, nausea, and vomiting for the past several months. The patient does not see a physician typically and has no known past medical history. He works as a farmer and interacts with livestock and also breeds dogs. His temperature is 98.7°F (37.1°C), blood pressure is 159/90 mmHg, pulse is 88/min, respirations are 15/min, and oxygen saturation is 99% on room air. Physical exam is notable for mild abdominal distension and discomfort to palpation of the upper abdominal quadrants. Laboratory values are ordered and are notable for a mild eosinophilia. A CT scan of the abdomen demonstrates multiple small eggshell calcifications within the right lobe of the liver. Which of the following is the most likely etiology of this patient's symptoms?
A 29-year-old woman comes to the military physician because of a 2-day history of fever, joint pain, dry cough, chest pain, and a painful red rash on her lower legs. Two weeks ago, she returned from military training in Southern California. She appears ill. Her temperature is 39°C (102.1°F). Physical examination shows diffuse inspiratory crackles over all lung fields and multiple tender erythematous nodules over the anterior aspect of both legs. A biopsy specimen of this patient's lungs is most likely to show which of the following?
A 42-year-old man comes to the physician because of a 3-week history of rash that began on his right ankle and gradually progressed up his calf. The rash is itchy and mildly painful. He has type 2 diabetes mellitus and hypertension. He does not smoke or drink alcohol. His current medications include metformin, glipizide, and enalapril. He returned from a trip to Nigeria around 5 weeks ago. He works on a fishing trawler. His temperature is 37°C (98.6°F), pulse is 65/min, and blood pressure is 150/86 mm Hg. Other than the rash on his calf, the examination shows no abnormalities. A picture of the rash is shown. Which of the following is the most likely cause of this patient's symptoms?

A 16-year-old male with no significant past medical, surgical, or family history presents to his pediatrician with new symptoms following a recent camping trip. He notes that he went with a group of friends and 1 other group member is experiencing similar symptoms. Over the past 5 days, he endorses significant flatulence, nausea, and greasy, foul-smelling diarrhea. He denies tenesmus, urgency, and bloody diarrhea. The blood pressure is 118/74 mm Hg, heart rate is 88/min, respiratory rate is 14/min, and temperature is 37.0°C (98.6°F). Physical examination is notable for mild, diffuse abdominal tenderness. He has no blood in the rectal vault. What is the patient most likely to report about his camping activities?
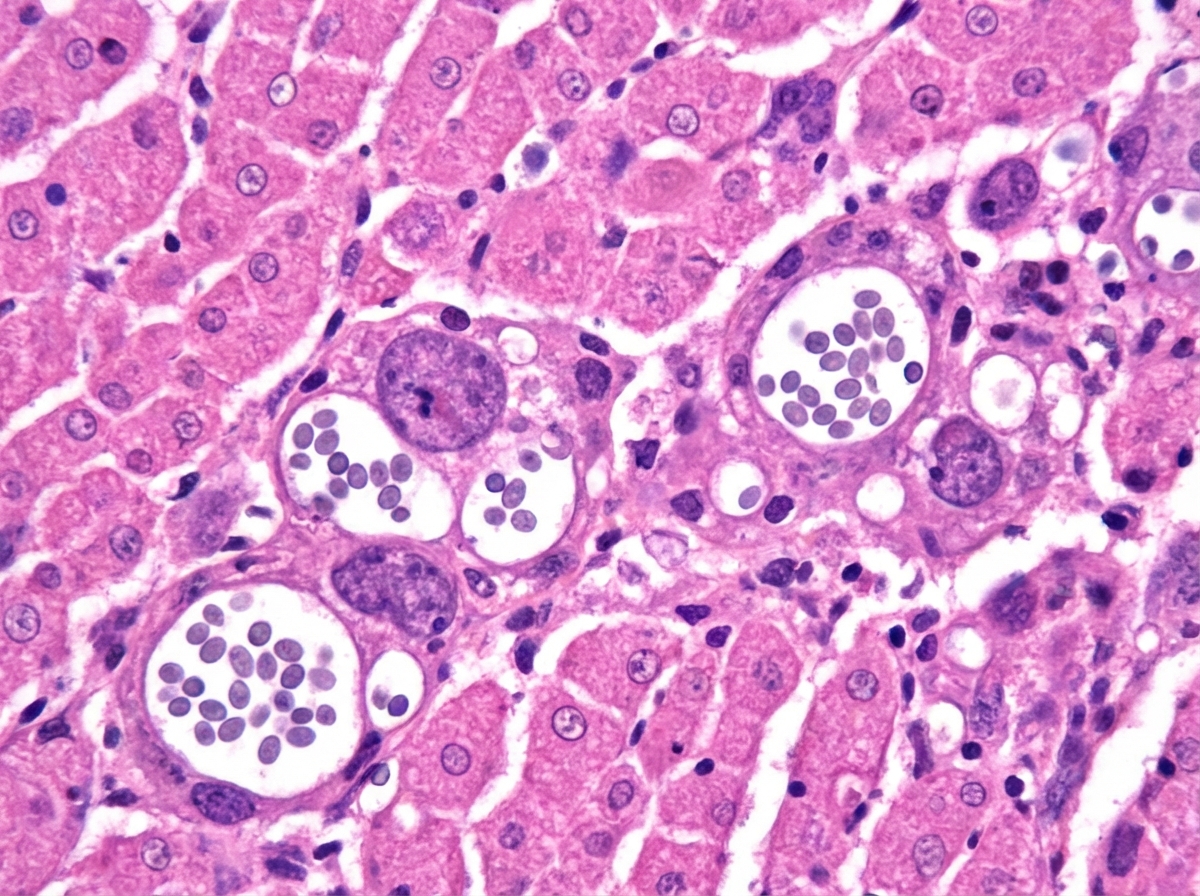
A 55-year-old man comes to the physician because of fever, fatigue, dry cough, headache, and myalgia over the past week. Two days ago, he developed several painful oral lesions and difficulty swallowing. He underwent kidney transplantation 3 years ago. His temperature is 38.2°C (100.7°F). Physical examination shows bilateral rales, hepatosplenomegaly, and multiple 1–2 cm ulcerative lesions with raised borders in the oral mucosa. A photomicrograph of a liver biopsy specimen is shown. Which of the following is the most likely causal pathogen?
Practice by Chapter
Candida species
Practice Questions
Aspergillus species
Practice Questions
Cryptococcus neoformans/gattii
Practice Questions
Pneumocystis jirovecii
Practice Questions
Mucormycoses
Practice Questions
Dermatophytes
Practice Questions
Antifungal agents
Practice Questions
Opportunistic fungal infections
Practice Questions
Parasitic life cycles
Practice Questions
Soil-transmitted helminths
Practice Questions
Filarial nematodes
Practice Questions
Schistosomiasis
Practice Questions
Echinococci and other tissue helminths
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app