
Parasites/Fungi — MCQs

On this page
A 34-year-old man comes to the physician because of progressive swelling of the left lower leg for 4 months. One year ago, he had an episode of intermittent fever and tender lymphadenopathy that occurred shortly after he returned from a trip to India and resolved spontaneously. Physical examination shows 4+ nonpitting edema of the left lower leg. His leukocyte count is 8,000/mm3 with 25% eosinophils. A blood smear obtained at night confirms the diagnosis. Treatment with diethylcarbamazine is initiated. Which of the following is the most likely route of transmission of the causal pathogen?
A 10-year-old girl presents to the clinic, with her mother, complaining of a circular, itchy rash on her scalp for the past 3 weeks. Her mother is also worried about her hair loss. The girl has a past medical history significant for asthma. She needs to use her albuterol inhaler once per week on average. Her blood pressure is 112/70 mm Hg; the heart rate is 104/min; the respiratory rate is 20/min, and the temperature is 37.0°C (98.6°F). On exam, the patient is alert and interactive. Her lungs are clear on bilateral auscultation. On palpation, a tender posterior cervical node is present on the right side. Examination of the head is shown in the image. Which of the following is the best treatment option for the patient?

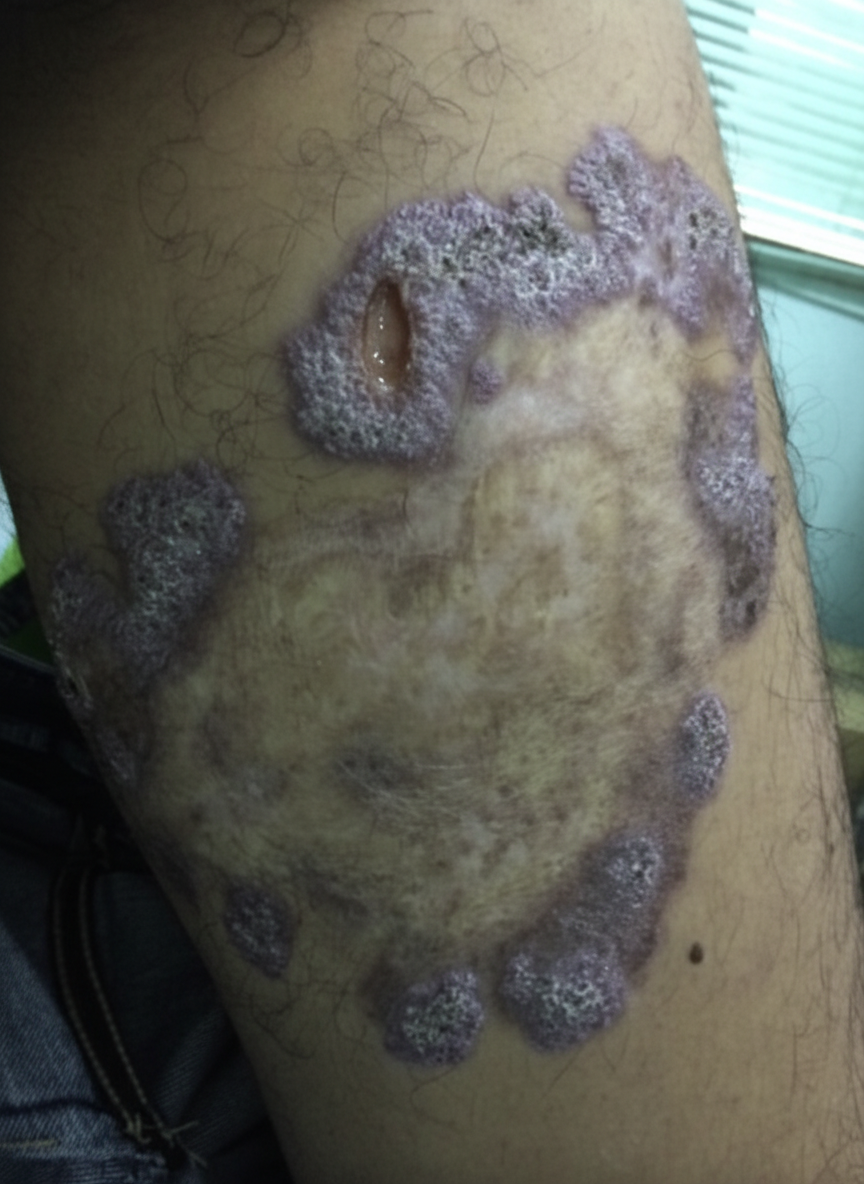
A 54-year-old gardener with diabetes mellitus from the Northeast Jilin Province in China acquired a small scratch from a thorn while working in his flower garden. After 3 weeks, he noticed a small pink, painless bump at the site of a scratch. He was not concerned by the bump; however, additional linearly-distributed bumps that resembled boils began to appear 1 week later that were quite painful. When the changes took on the appearance of open sores that drained clear fluid without any evidence of healing (as shown on the image), he finally visited his physician. The physician referred to the gardener for a skin biopsy to confirm his working diagnosis and to start treatment as soon as possible. Which of the following is the most likely diagnosis for this patient?
A 21-year-old woman comes to the physician because of a 1-week history of white discoloration of the tongue. She has had similar, recurrent episodes over the past 5 years. Examination shows white plaques on the tongue that easily scrape off and thick, cracked fingernails with white discoloration. KOH preparation of a tongue scraping shows budding yeasts with pseudohyphae. This patient's condition is most likely caused by decreased activity of which of the following?
A 26-year-old man with HIV and a recent CD4+ count of 800 presents to his PCP with fever, cough, and dyspnea. He notes that he recently lost his job as a construction worker and has not been able to afford his HAART medication. His temperature is 102.6°F (39.2°C), pulse is 75/min, respirations are 24/min, and blood pressure is 135/92 mmHg. Physical exam reveals a tachypneic patient with scattered crackles in both lungs, and labs show a CD4+ count of 145 and an elevated LDH. The chest radiography is notable for bilateral diffuse interstitial infiltrates. For definitive diagnosis, the physician obtains a sputum sample. Which stain should he use to visualize the most likely responsible organism?
A 2900-g (6.4-lb) male newborn is delivered at term to a 29-year-old primigravid woman. His mother had no routine prenatal care. She reports that the pregnancy was uncomplicated apart from a 2-week episode of a low-grade fever and swollen lymph nodes during her early pregnancy. She has avoided all routine vaccinations because she believes that “natural immunity is better.” The newborn is at the 35th percentile for height, 15th percentile for weight, and 3rd percentile for head circumference. Fundoscopic examination shows inflammation of the choroid and the retina in both eyes. A CT scan of the head shows diffuse intracranial calcifications and mild ventriculomegaly. Prenatal avoidance of which of the following would have most likely prevented this newborn's condition?
An investigator studying fungal growth isolates organisms from an infant with diaper rash. The isolate is cultured and exposed to increasing concentrations of nystatin. Selected colonies continue to grow and replicate even at high concentrations of the drug. Which of the following is the most likely explanation for this finding?
A 16-year-old girl presents to her physician with itching, soreness, and irritation in the vulvar region. She reports that these episodes have occurred 6–7 times a year since the age of 5. She used to treat these symptoms with topical ketoconazole cream, but this time it failed to help. She also has had several episodes of oral candidiasis in the past. She is not sexually active and does not take any medication. Her vital signs are as follows: the blood pressure is 115/80 mm Hg, the heart rate is 78/min, the respiratory rate is 15/min, and the temperature is 35.5°C (97.7°F). Examination shows vulvovaginal erythema with cottage cheese-like plaques and an intact hymen. Wet mount microscopy is positive for yeast. Along with a swab culture, the physician orders a dihydrorhodamine test and myeloperoxidase staining for a suspected primary immunodeficiency. The dihydrorhodamine test is positive, and the myeloperoxidase staining reveals diminished staining. Which of the following best describes this patient's condition?
Four days after undergoing liver transplantation, a 47-year-old man develops fever, chills, malaise, and confusion while in the intensive care unit. His temperature is 39.1°C (102.4°F). Blood cultures grow an organism. Microscopic examination of this organism after incubation at 37°C (98.6°F) for 3 hours is shown. Which of the following is the most likely causal organism of this patient's symptoms?

A 31-year-old man living in a remote tropical village presents with a swollen left leg and scrotum (see image). He says that his symptoms started more than 2 years ago with several small swollen areas near his groin and have gradually and progressively worsened. He has also noticed that over time, there has been a progressive coarsening and fissuring of the skin overlying the swollen areas. Blood samples drawn at night show worm-like organisms under microscopy. Which of the following arthropods is the vector for the organism most likely responsible for this patient’s condition?

Practice by Chapter
Candida species
Practice Questions
Aspergillus species
Practice Questions
Cryptococcus neoformans/gattii
Practice Questions
Pneumocystis jirovecii
Practice Questions
Mucormycoses
Practice Questions
Dermatophytes
Practice Questions
Antifungal agents
Practice Questions
Opportunistic fungal infections
Practice Questions
Parasitic life cycles
Practice Questions
Soil-transmitted helminths
Practice Questions
Filarial nematodes
Practice Questions
Schistosomiasis
Practice Questions
Echinococci and other tissue helminths
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app