
Parasites/Fungi — MCQs

On this page
A 52-year-old man presents with a 5-week history of multiple cutaneous ulcers on his left forearm and neck, which he first noticed after returning from a 2-month stay in rural Peru. He does not recall any trauma or arthropod bites. The lesions began as non-pruritic erythematous papules that became enlarged, ulcerated, and crusted. There is no history of fever or abdominal pain. He has been sexually active with a single partner since their marriage at 24 years of age. The physical examination reveals erythematous, crusted plaques with central ulceration and a raised border. There is no fluctuance, drainage, or sporotrichoid spread. A punch biopsy was performed, which revealed an ulcerated lesion with a mixed inflammatory infiltrate. Amastigotes within dermal macrophages are seen on Giemsa staining. What is the most likely diagnosis?
A 48-year-old man comes to the physician for evaluation of an intensely pruritic skin rash on his arms and legs for 12 hours. Two days ago, he returned from an annual camping trip with his son. The patient takes no medications. A photograph of the skin lesions on his left hand is shown. Activation of which of the following cell types is the most likely cause of this patient's skin findings?

A 27-year-old female presents to her primary care physician because she is concerned about lighter colored patches on her skin. She recently went sunbathing and noticed that these areas also did not tan. Her doctor explains that she has a fungal infection of the skin that damages melanocytes by producing acids. She is prescribed selenium sulfide and told to follow-up in one month. Which of the following describes the appearance of the most likely infectious organism under microscopy?
A 42-year-old woman comes to the physician because of episodic abdominal pain and fullness for 1 month. She works as an assistant at an animal shelter and helps to feed and bathe the animals. Physical examination shows hepatomegaly. Abdominal ultrasound shows a 4-cm calcified cyst with several daughter cysts in the liver. She undergoes CT-guided percutaneous aspiration under general anesthesia. Several minutes into the procedure, one liver cyst spills, and the patient's oxygen saturation decreases from 95% to 64%. Her pulse is 136/min, and blood pressure is 86/58 mm Hg. Which of the following is the most likely causal organism of this patient's condition?
A 4-year-old girl presents with recurrent abdominal pain and a low-grade fever for the past 2 months. The patient’s mother says that she has lost her appetite which has caused some recent weight loss. She adds that the patient frequently plays outdoors with their pet dog. The patient is afebrile and vital signs are within normal limits. On physical examination, conjunctival pallor is present. Abdominal examination reveals a diffusely tender abdomen and significant hepatomegaly. There is also a solid mass palpable in the right upper quadrant measuring about 3 x 4 cm. Laboratory findings are significant for the following: Hemoglobin (Hb%) 9.9 g/dL Total count (WBC) 26,300/µL Differential count Neutrophils 36% Lymphocytes 16% Eosinophils 46% Platelets 200,000/mm3 Erythrocyte sedimentation rate 56 mm/h C-reactive protein 2 mg/L Serum globulins 5 g/dL Laparoscopic resection of the mass is performed, and a tissue sample is sent for histopathology. Which of the following is the organism most likely responsible for this patient’s condition?
A 65-year-old woman who lives in New York City presents with headache, fever, and neck stiffness. She received a diagnosis of HIV infection 3 years ago and has been inconsistent with her antiretroviral medications. A computed tomography of her head is normal. A lumbar puncture shows a white blood cell count of 45/mm3 with a mononuclear predominance, the glucose level of 30 mg/dL, and a protein level of 60 mg/dL. A preparation of her cerebrospinal fluid is shown. Which of the following organisms is the most likely cause of her symptoms?
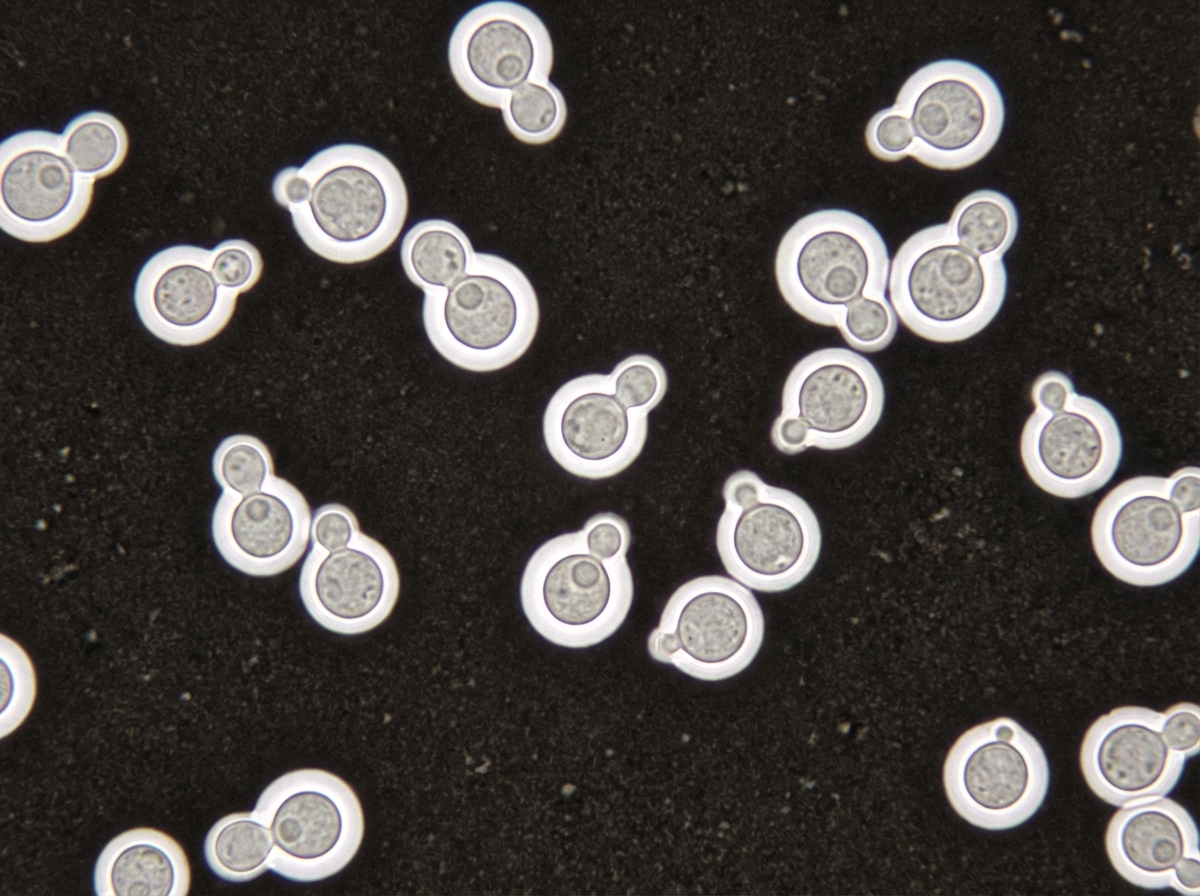
A 3-month-old girl is brought to the emergency department because of a 2-day history of progressive difficulty breathing and a dry cough. Five weeks ago, she was diagnosed with diffuse hemangiomas involving the intrathoracic cavity and started treatment with prednisolone. She appears uncomfortable and in moderate respiratory distress. Her temperature is 38°C (100.4°F), pulse is 150/min, respirations are 50/min, and blood pressure is 88/50 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 87%. Oral examination shows a white plaque covering the tongue that bleeds when scraped. Chest examination shows subcostal and intercostal retractions. Scattered fine crackles and rhonchi are heard throughout both lung fields. Laboratory studies show a leukocyte count of 21,000/mm3 and an increased serum beta-D-glucan concentration. An x-ray of the chest shows symmetrical, diffuse interstitial infiltrates. Which of the following is most likely to confirm the diagnosis?
A 43-year-old type 1 diabetic woman who is poorly compliant with her diabetes medications presented to the emergency department with hemorrhage from her nose. On exam, you observe the findings shown in figure A. What is the most likely explanation for these findings?

A 7-year-old boy with a history of cystic fibrosis is brought to the physician for evaluation of recurrent episodes of productive cough, wheezing, and shortness of breath over the past month. Physical examination shows coarse crackles and expiratory wheezing over both lung fields. Serum studies show elevated levels of IgE and eosinophilia. A CT scan of the lungs shows centrally dilated bronchi with thickened walls and peripheral airspace consolidation. Antibiotic therapy is initiated. One week later, the patient continues to show deterioration in lung function. A sputum culture is most likely to grow which of the following?
A 12-year-old child is exposed to pollen while playing outside. The allergen stimulates TH2 cells of his immune system to secrete a factor that leads to B-cell class switching to IgE. What factor is secreted by the TH2 cell?
Practice by Chapter
Candida species
Practice Questions
Aspergillus species
Practice Questions
Cryptococcus neoformans/gattii
Practice Questions
Pneumocystis jirovecii
Practice Questions
Mucormycoses
Practice Questions
Dermatophytes
Practice Questions
Antifungal agents
Practice Questions
Opportunistic fungal infections
Practice Questions
Parasitic life cycles
Practice Questions
Soil-transmitted helminths
Practice Questions
Filarial nematodes
Practice Questions
Schistosomiasis
Practice Questions
Echinococci and other tissue helminths
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app