
Parasites/Fungi — MCQs

On this page
A 47-year-old man presents to the emergency department with jaundice and extreme fatigue for the past 4 days. He also noticed that his stool is very pale and urine is dark. Past medical history is unremarkable. The review of systems is significant for a 23 kg (50 lb) weight loss over the last 3 months which he says is due to decreased appetite. He is afebrile and the vital signs are within normal limits. A contrast computed tomography (CT) scan of the abdomen reveals a mass in the pancreatic head. A blood test for carbohydrate antigen (CA19-9) is positive. The patient is admitted to the intensive care unit (ICU) and undergoes surgical decompression of the biliary tract. He is placed on total parenteral nutrition (TPN). On day 4 after admission, his intravenous access site is found to be erythematous and edematous. Which of the following microorganisms is most likely responsible for this patient’s intravenous (IV) site infection?
A 9-year-old girl is brought to the pediatrician by her mother who reports that the girl has been complaining of genital itching over the past few days. She states she has noticed her daughter scratching her buttocks and anus for the past week; however, now she is scratching her groin quite profusely as well. The mother notices that symptoms seem to be worse at night. The girl is otherwise healthy, is up to date on her vaccinations, and feels well. She was recently treated with amoxicillin for a middle ear infection. The child also had a recent bout of diarrhea that was profuse and watery that seems to be improving. Her temperature is 98.5°F (36.9°C), blood pressure is 111/70 mmHg, pulse is 83/min, respirations are 16/min, and oxygen saturation is 98% on room air. Physical exam is notable for excoriations over the girl's anus and near her vagina. Which of the following is the most likely infectious etiology?
A 30-year-old man is admitted to the hospital with a presumed pneumonia and started on antibiotics. Two days later, the patient shows no improvement. Blood cultures reveal yeast with pseudophyphae. Which of the following cell types is most likely deficient or dysfunctional in this patient?
A 3-month-old boy is brought to the physician by his parents because of a 2-day history of poor feeding and lethargy. He was born at term and has had three episodes of bilateral otitis media since birth. Umbilical cord separation occurred at the age of 8 weeks. He is at the 30th percentile for height and 20th percentile for weight. His temperature is 39°C (102.2°F) and blood pressure is 58/36 mm Hg. Physical examination shows white oral patches and confluent scaly erythematous skin lesions in the groin. Laboratory studies show a leukocyte count of 41,300/mm3 (92% segmented neutrophils and 8% lymphocytes) and a platelet count of 224,000/mm3. Blood cultures at 20°C (68°F) grow catalase-positive yeast cells that form pseudohyphae. Which of the following is the most likely underlying cause of this patient's symptoms?
A 30-year-old man presents to the physician after he discovered a raised, red, string-shaped lesion beneath the skin on his right foot. The lesion seems to move from one location to another over the dorsum of his foot from day to day. He says that the lesion is extremely itchy and has not responded to over the counter topical treatment. He and his wife recently returned from a honeymoon in southern Thailand, where they frequented the tropical beaches. The physician diagnoses him with a parasitic infection and prescribes albendazole for the patient. With which of the following organisms is the patient most likely infected?
A 50-year-old HIV-positive male presents to the ER with a two-day history of fever and hemoptysis. Chest radiograph shows a fibrocavitary lesion in the right middle lobe. Biopsy of the afflicted area demonstrates septate hyphae that branch at acute angles. Which of the following is the most likely causal organism?
A 31-year-old female undergoing treatment for leukemia is found to have a frontal lobe abscess accompanied by paranasal swelling. She additionally complains of headache, facial pain, and nasal discharge. Biopsy of the infected tissue would most likely reveal which of the following?
A 68-year-old man presents to his physician for symptoms of chronic weight loss, abdominal bloating, and loose stools. He notes that he has also been bothered by a chronic cough. The patient’s laboratory work-up includes a WBC differential, which is remarkable for an eosinophil count of 9%. Stool samples are obtained, with ova and parasite examination revealing roundworm larvae in the stool and no eggs. Which of the following parasitic worms is the cause of this patient’s condition?
A 3-year-old boy is brought to his pediatrician by his mother for a productive cough. His symptoms began approximately 3 days prior to presentation and have not improved. His mother also reports that he developed diarrhea recently and denies any sick contacts or recent travel. He has received all of his vaccinations. Medical history is significant for pneumonia and a lung abscess of staphylococcal origin, and osteomyelitis caused by Serratia marcescens. Physical examination demonstrates growth failure and dermatitis. Laboratory testing is remarkable for hypergammaglobulinemia and a non-hemolytic and normocytic anemia. Work-up of his productive cough reveals that it is pneumonia caused by Aspergillus fumigatus. Which of the following is most likely the immune system defect that will be found in this patient?
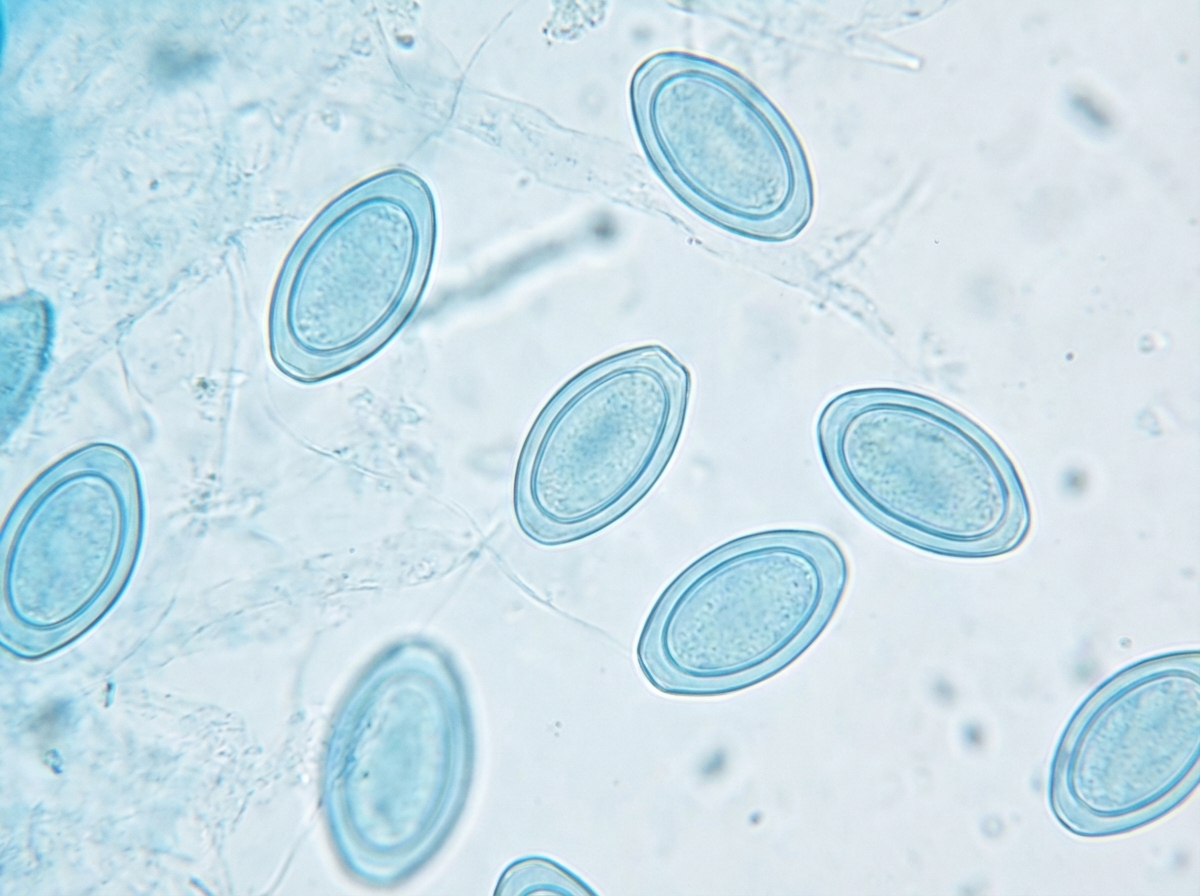
A 2-year-old girl is brought to the doctor by her mother with persistent scratching of her perianal region. The patient's mother says that symptoms started 3 days ago and have progressively worsened until she is nearly continuously scratching even in public places. She says that the scratching is worse at night and disturbs her sleep. A perianal adhesive tape test is performed and direct microscopy reveals findings in the image (see image). Which of the following is the organism most likely responsible for this patient's condition?
Practice by Chapter
Candida species
Practice Questions
Aspergillus species
Practice Questions
Cryptococcus neoformans/gattii
Practice Questions
Pneumocystis jirovecii
Practice Questions
Mucormycoses
Practice Questions
Dermatophytes
Practice Questions
Antifungal agents
Practice Questions
Opportunistic fungal infections
Practice Questions
Parasitic life cycles
Practice Questions
Soil-transmitted helminths
Practice Questions
Filarial nematodes
Practice Questions
Schistosomiasis
Practice Questions
Echinococci and other tissue helminths
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app