
Parasites/Fungi — MCQs

On this page
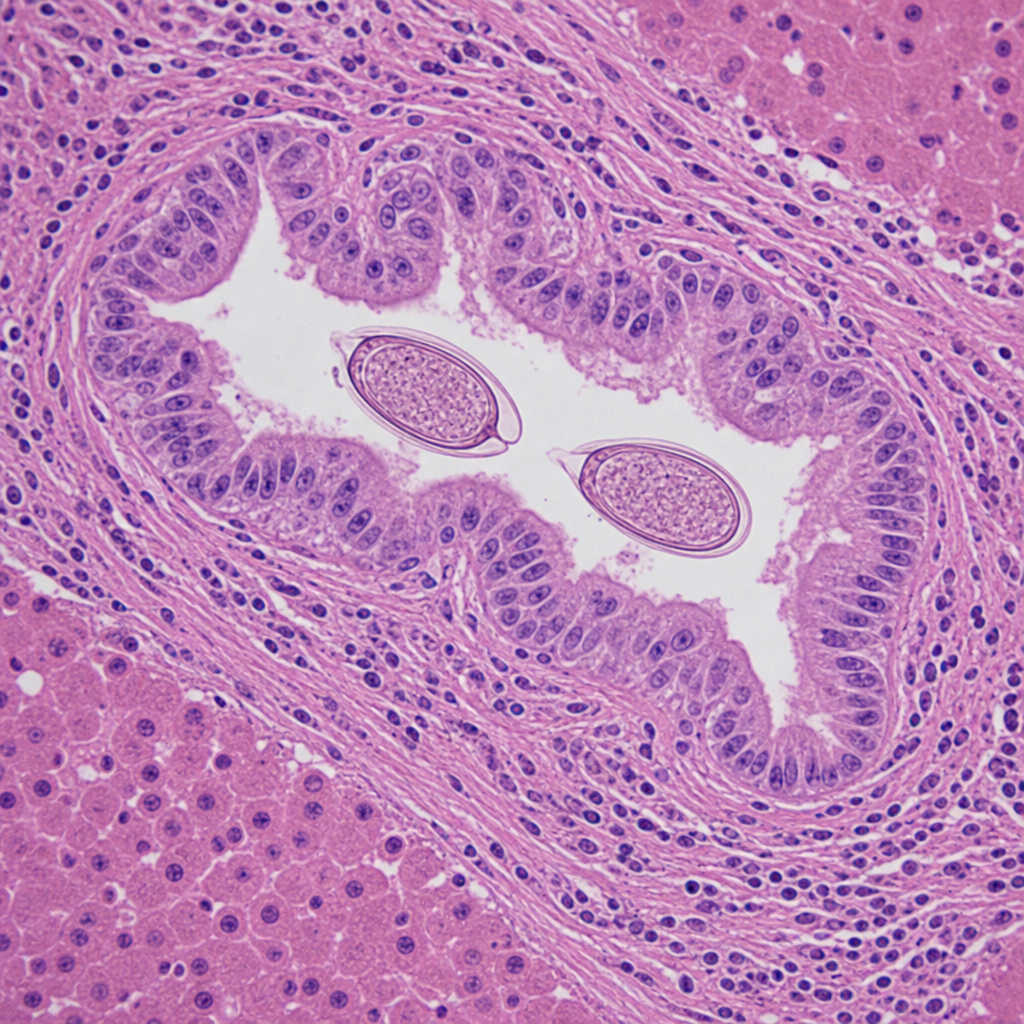
A photomicrograph shows a liver biopsy specimen from a 45-year-old Southeast Asian immigrant with chronic fatigue and right upper quadrant discomfort. The hematoxylin and eosin-stained section reveals intrahepatic bile duct epithelium with marked hyperplasia and periductal fibrosis. Within the bile duct lumen, elongated, operculated eggs measuring approximately 29 × 16 µm are visible. Serological testing is positive. Which of the following organisms is most consistent with these findings?
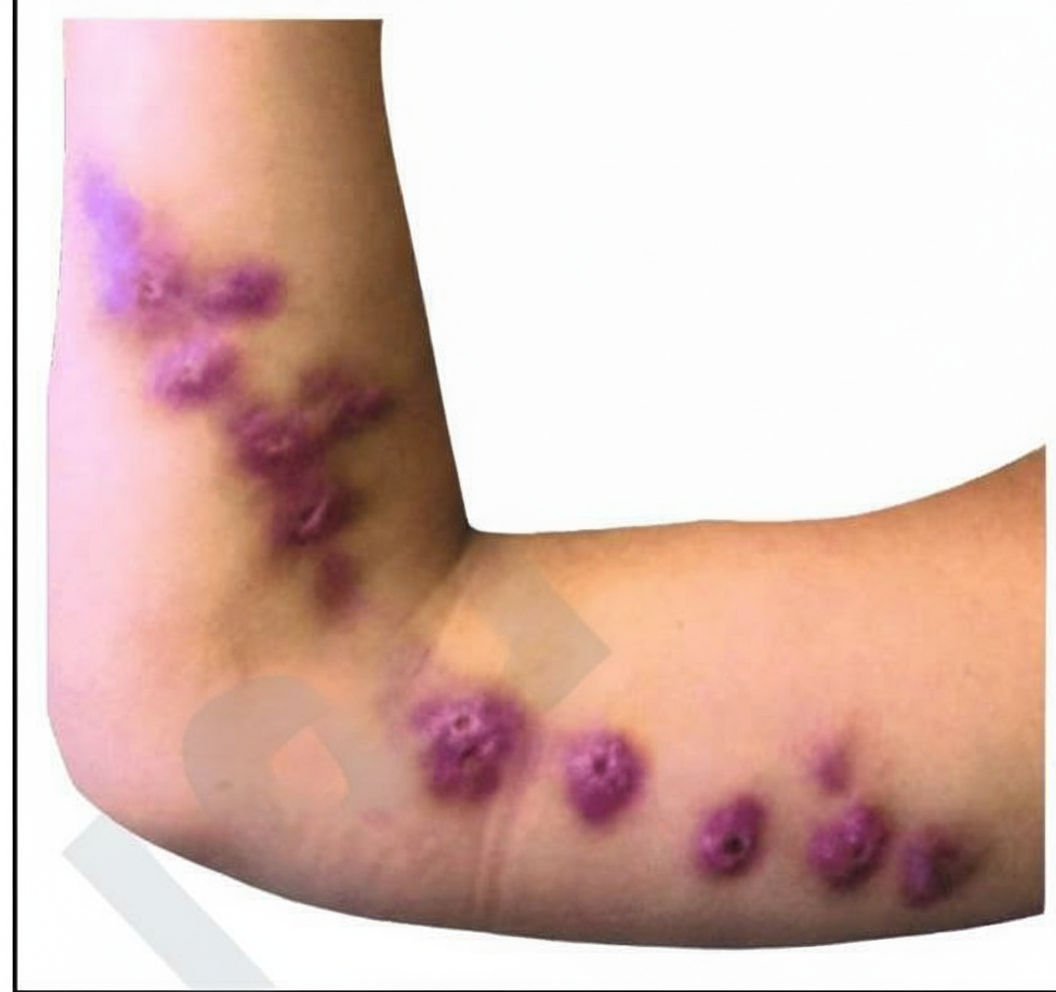
A previously healthy 48-year-old man comes to the physician because of a 2-week history of a nonpruritic rash on his right forearm. The rash began as pustules and progressed to form nodules and ulcers. He works as a gardener. Physical examination shows right axillary lymphadenopathy and the findings in the photograph. Which of the following is the most likely causal organism?
A 29-year-old internal medicine resident presents to the emergency department with complaints of fevers, diarrhea, abdominal pain, and skin rash for 2 days. He feels fatigued and has lost his appetite. On further questioning, he says that he returned from his missionary trip to Brazil last week. He is excited as he talks about his trip. Besides a worthy clinical experience, he also enjoyed local outdoor activities, like swimming and rafting. His past medical history is insignificant. The blood pressure is 120/70 mm Hg, the pulse is 100/min, and the temperature is 38.3°C (100.9°F). On examination, there is a rash on the legs. The rest of the examination is normal. Which of the following organisms is most likely responsible for this patient’s condition?
A 19-year-old woman presents to the emergency department with complaints of blurry vision and headaches that started 2 days ago. She reports that she has been experiencing some facial pain, but she thought it was related to her toothache. She is also worried about a black spot that is increasing in size on her face over the last month. She expresses concerns about her frequency of urination. Recently, she had a runny nose and cough that resolved spontaneously. The patient was diagnosed with type 1 diabetes mellitus at 13 years of age. She is a non-smoker and drinks beer occasionally. Her blood pressure is 122/98 mm Hg and temperature is 37.2°C (98.9°F). The physical examination is normal with the exception of a black necrotic eschar lateral to the right nasal ala. She lost 2.7 kg (6 lb) since her last visit, which was 6 months ago. A routine urinalysis at the office is positive for glucose and ketones. What is the most likely cause of the patient’s symptoms?
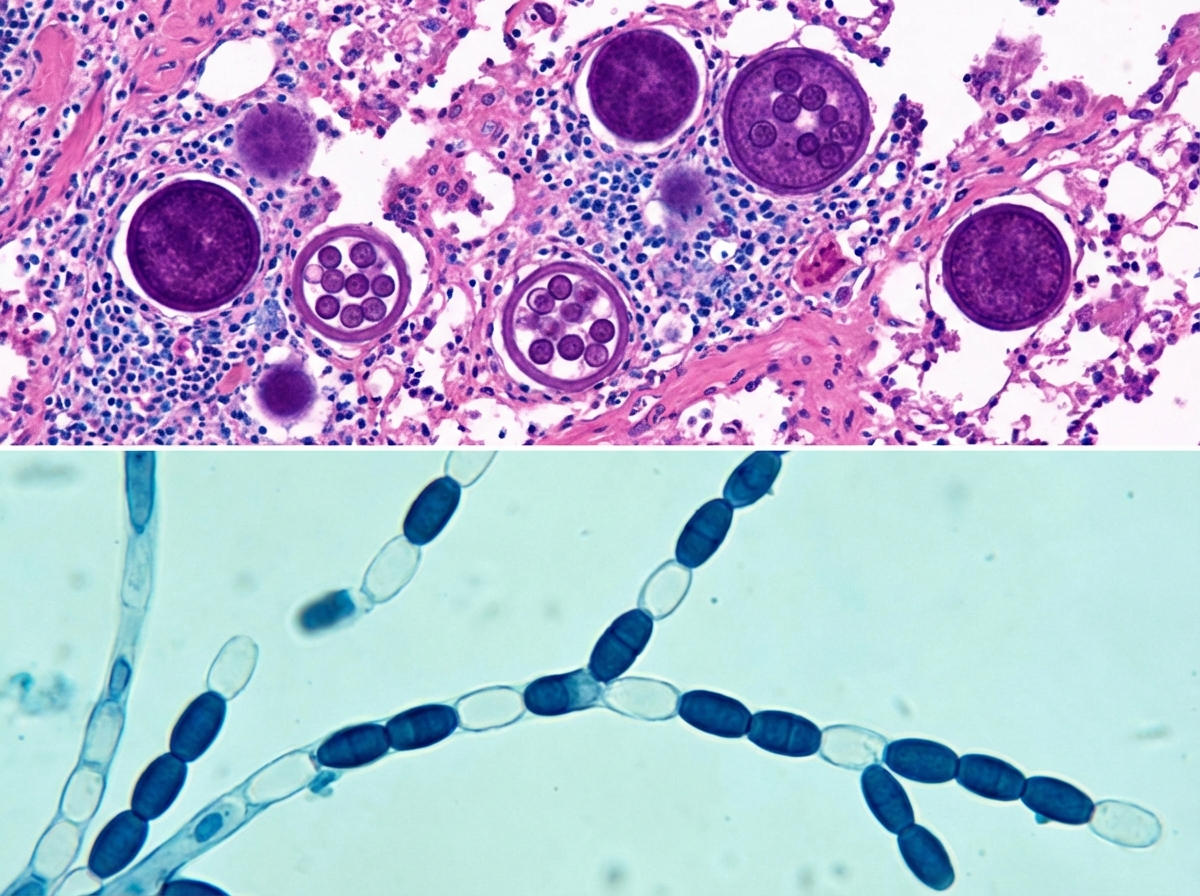
A 75-year-old man who underwent a bilateral lung transplant 11 months ago presented to the emergency room with fevers and chills. After the transplant procedure, he was immediately placed on immunosuppressive treatment; however, for unknown reasons he stopped taking the prophylactically-prescribed voriconazole (a triazole antifungal medication used for the treatment and prevention of invasive fungal infections). Upon presentation to the emergency room, the patient was hypoxemic. Imaging revealed pulmonary nodules, which prompted a transbronchial biopsy for further evaluation. The results were negative for acute organ rejection, adenovirus, cytomegalovirus, and acid-fast bacilli. Slides stained with hematoxylin and eosin (H&E) were also prepared, as presented on the upper panel of the accompanying picture, which revealed large round structures. The specimen was sent to the microbiology laboratory for fungal culture, which resulted in the growth of a fuzzy mold on Sabouraud agar (selective medium for the isolation of fungi) at 30.0°C (86.0°F). A lactophenol cotton blue preparation revealed the organism shown on the lower panel of the accompanying picture. What organism has infected this patient?
A 58-year-old man presents with a high-grade fever, throbbing left-sided headache, vision loss, and left orbital pain. He says that his symptoms started acutely 2 days ago with painful left-sided mid-facial swelling and a rash, which progressively worsened. Today, he woke up with complete vision loss in his left eye. His past medical history is significant for type 2 diabetes mellitus, diagnosed 5 years ago. He was started on an oral hypoglycemic agent which he discontinued after a year. His temperature is 38.9°C (102.0°F), blood pressure is 120/80 mm Hg, pulse is 120/min, and respiratory rate is 20/min. On examination, there is purulent discharge from the left eye and swelling of the left half of his face including the orbit. Oral examination reveals extensive necrosis of the palate with a black necrotic eschar and purulent discharge. Ophthalmic examination is significant for left-sided ptosis, proptosis, and an absence of the pupillary light reflex. Laboratory findings are significant for a blood glucose level of 388 mg/dL and a white blood cell count of 19,000 cells/mm³. Urinary ketone bodies are positive. Fungal elements are found on a KOH mount of the discharge. Which of the following statements best describes the organism responsible for this patient’s condition?
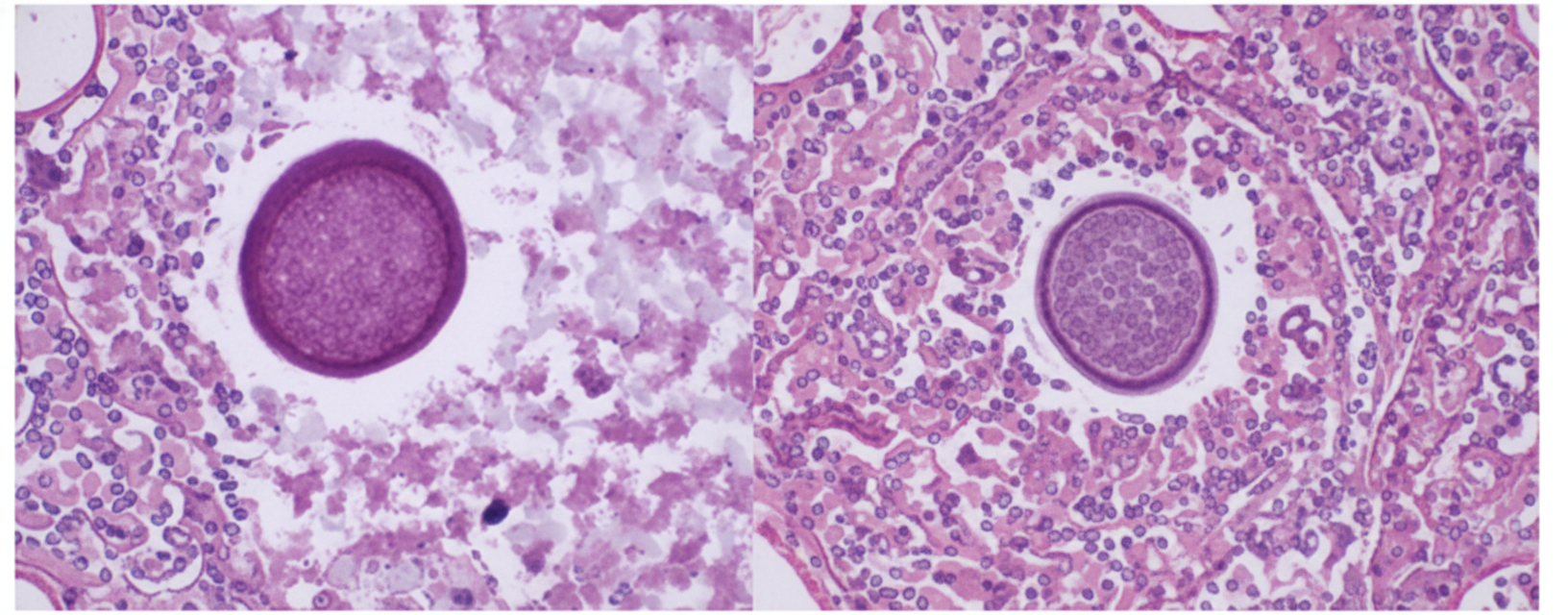
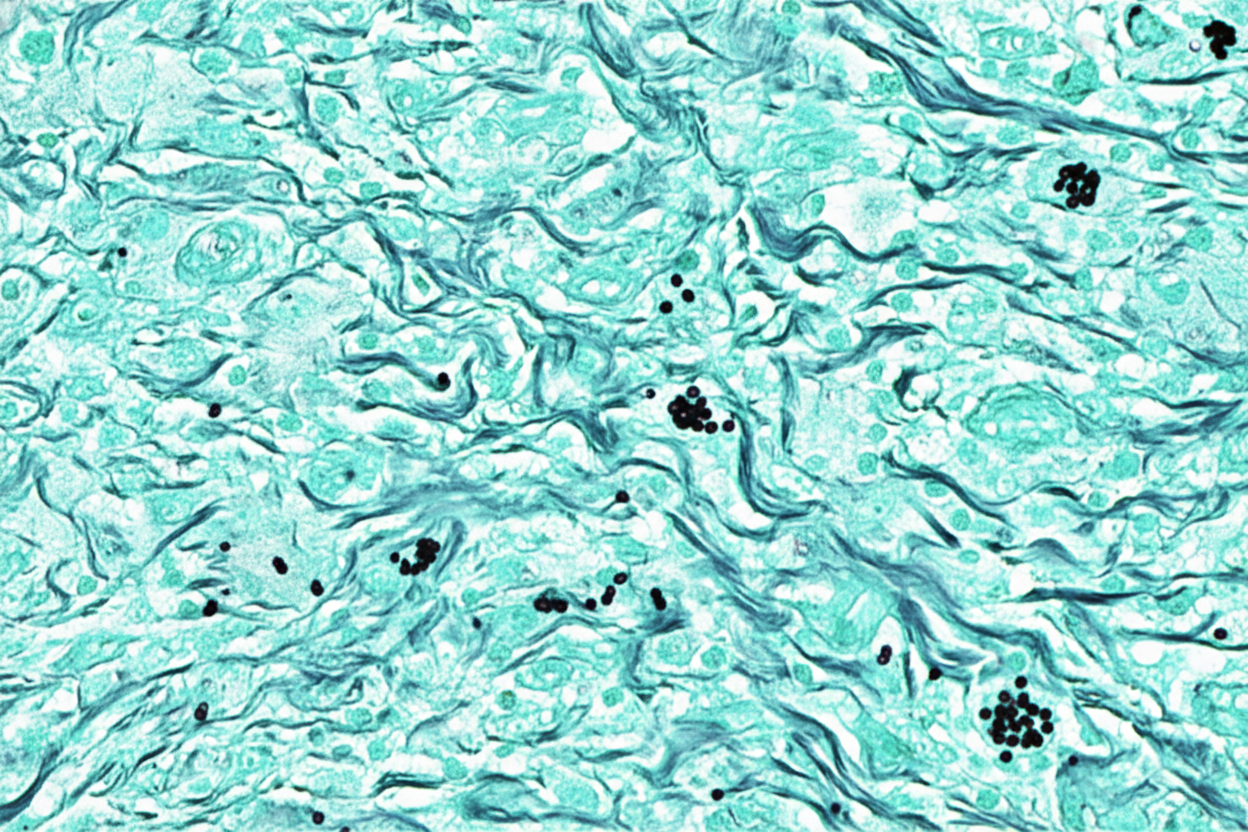
A 26-year-old female presents to the emergency department with high fever, productive cough, and hemoptysis. She says that she has also been getting red tender bumps under the skin as well as joint pain. She believes that her symptoms started a few days after a small earthquake hit near her hometown and was otherwise healthy prior to these symptoms. No pathogenic bacteria are detected on sputum culture or by Gram stain. Based on clinical suspicion a lung biopsy is performed and the results are shown in the image provided. The most likely pathogen causing this disease lives in which of the following locations?
A 4-month-old boy is brought to the physician by his father because of a progressively worsening rash on his buttocks for the last week. He cries during diaper changes and is more fussy than usual. Physical examination of the boy shows erythematous papules and plaques in the bilateral inguinal creases, on the scrotum, and in the gluteal cleft. Small areas of maceration are also present. A diagnosis is made, and treatment with topical clotrimazole is initiated. Microscopic examination of skin scrapings from this patient's rash is most likely to show which of the following findings?
A 22-year-old man comes to the physician because of abdominal pain, diarrhea, and weight loss that started after a recent backpacking trip in Southeast Asia. He does not smoke or drink alcohol. His leukocyte count is 7,500/mm3 (61% segmented neutrophils, 13% eosinophils, and 26% lymphocytes). Stool microscopy shows rhabditiform larvae. This patient is most likely to develop which of the following?
A 52-year-old man comes to the physician because of a 4-day history of a productive cough, shortness of breath, and low-grade fever. He works as a farmer in southern Arizona. Physical examination shows multiple skin lesions with a dark blue center, pale intermediate zone, and red peripheral rim on the upper and lower extremities. There are diffuse crackles on the left side of the chest. An x-ray of the chest shows left basilar consolidation and left hilar lymphadenopathy. A photomicrograph of tissue obtained from a biopsy of the lung is shown. Which of the following is the most likely causal pathogen?
Practice by Chapter
Candida species
Practice Questions
Aspergillus species
Practice Questions
Cryptococcus neoformans/gattii
Practice Questions
Pneumocystis jirovecii
Practice Questions
Mucormycoses
Practice Questions
Dermatophytes
Practice Questions
Antifungal agents
Practice Questions
Opportunistic fungal infections
Practice Questions
Parasitic life cycles
Practice Questions
Soil-transmitted helminths
Practice Questions
Filarial nematodes
Practice Questions
Schistosomiasis
Practice Questions
Echinococci and other tissue helminths
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app