
Human papillomavirus — MCQs

A 56-year-old woman makes an appointment with her physician to discuss the results of her cervical cancer screening. She has been menopausal for 2 years and does not take hormone replacement therapy. Her previous Pap smear showed low-grade squamous intraepithelial lesion (LSIL); no HPV testing was performed. Her gynecologic examination is unremarkable. The results of her current Pap smear is as follows: Specimen adequacy satisfactory for evaluation Interpretation low-grade squamous intraepithelial lesion Notes atrophic pattern Which option is the next best step in the management of this patient?
Researchers are investigating a new strain of a virus that has been infecting children over the past season and causing dermatitis. They have isolated the virus and have run a number of tests to determine its structure and characteristics. They have found that this new virus has an outer coating that is high in phospholipids. Protein targeting assays and immunofluorescence images have shown that the outer layer contains numerous surface proteins. On microscopy, these surface proteins are also expressed around the nucleus of cells derived from the infected tissue of the children. This virus’s structure most closely resembles which of the following?
A 31-year-old female presents to her gynecologist for a routine Pap smear. Her last Pap smear was three years ago and was normal. On the current Pap smear, she is found to have atypical squamous cells of unknown significance (ASCUS). Reflex HPV testing is positive. What is the best next step?
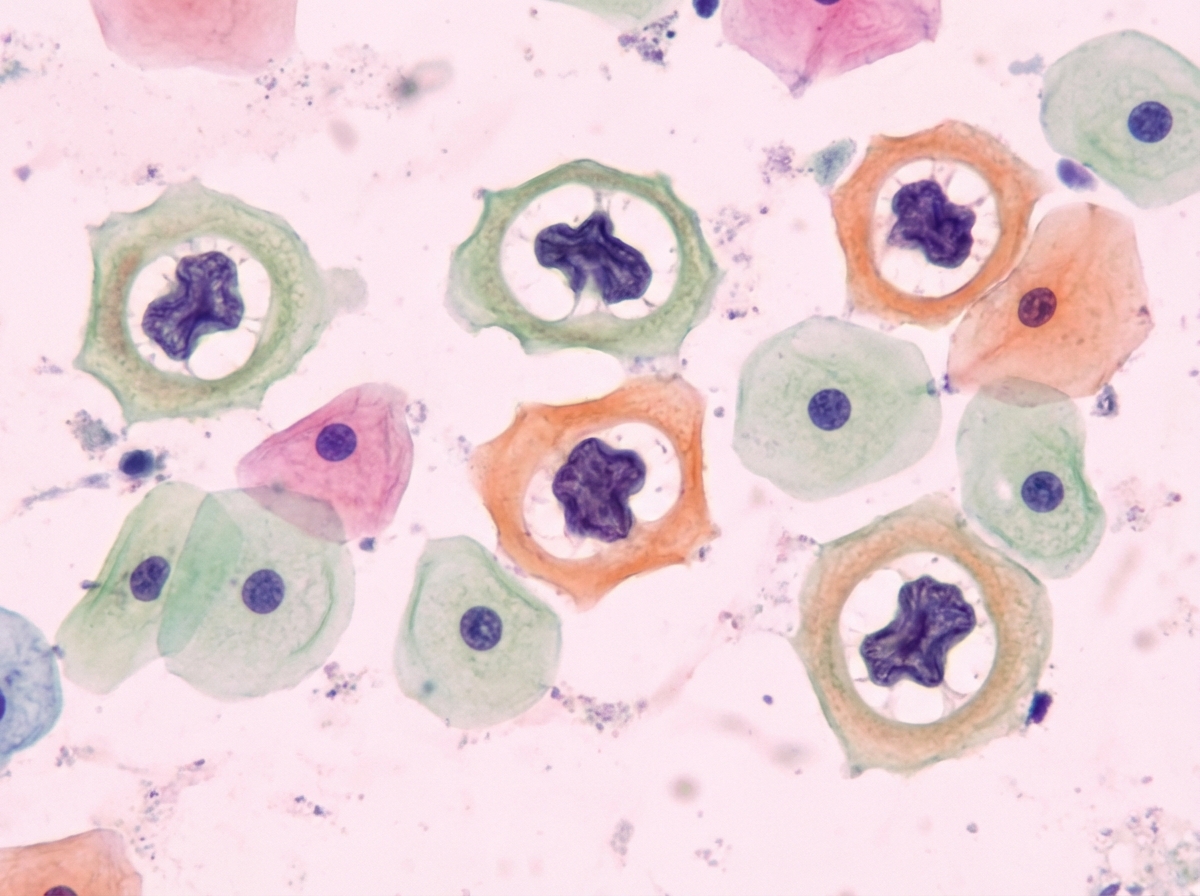
A 36-year-old woman comes to the physician for an annual pelvic examination and Pap smear. Her last Pap smear was 3 years ago. She has been sexually active with multiple male partners and takes an oral contraceptive. She has smoked one pack of cigarettes daily for 10 years. Pelvic examination shows no abnormalities. A photomicrograph of cervical cells from the Pap smear specimen is shown. Cells similar to the one indicated by the arrow are most likely to be seen in which of the following conditions?
A 55-year-old postmenopausal woman comes to the physician for a screening Pap smear. She has no history of serious illness. Her last Pap smear was 10 years ago and showed no abnormalities. She has smoked one-half pack of cigarettes daily for 20 years and drinks 3 bottles of wine per week. She is sexually active with multiple male partners and uses condoms inconsistently. Her paternal grandmother had ovarian cancer and her maternal aunt had breast cancer. Pelvic examination shows multiple red, fleshy polypoid masses on the anterior vaginal wall. A biopsy is obtained and histology shows large cells with abundant clear cytoplasm. Which of the following is the most significant risk factor for this diagnosis?
A 34-year-old G2P2 undergoes colposcopy due to high-grade intraepithelial neoplasia detected on a Pap smear. Her 2 previous Pap smears showed low-grade intraepithelial neoplasia. She has had 2 sexual partners in her life, and her husband has been her only sexual partner for the last 10 years. She had her sexual debut at 16 years of age. She had her first pregnancy at 26 years of age. She uses oral contraceptives for birth control. Her medical history is significant for right ovary resection due to a large follicular cyst and cocaine abuse for which she completed a rehabilitation program. Colposcopy reveals an acetowhite lesion with distorted vascularity at 4 o'clock. Which of the following factors present in this patient is a risk factor for the detected condition?
A 27-year-old woman comes to the physician for a routine health maintenance examination. She feels well. She had a chlamydia infection at the age of 22 years that was treated. Her only medication is an oral contraceptive. She has smoked one pack of cigarettes daily for 6 years. She has recently been sexually active with 3 male partners and uses condoms inconsistently. Her last Pap test was 4 years ago and results were normal. Physical examination shows no abnormalities. A Pap test shows atypical squamous cells of undetermined significance. Which of the following is the most appropriate next step in management?
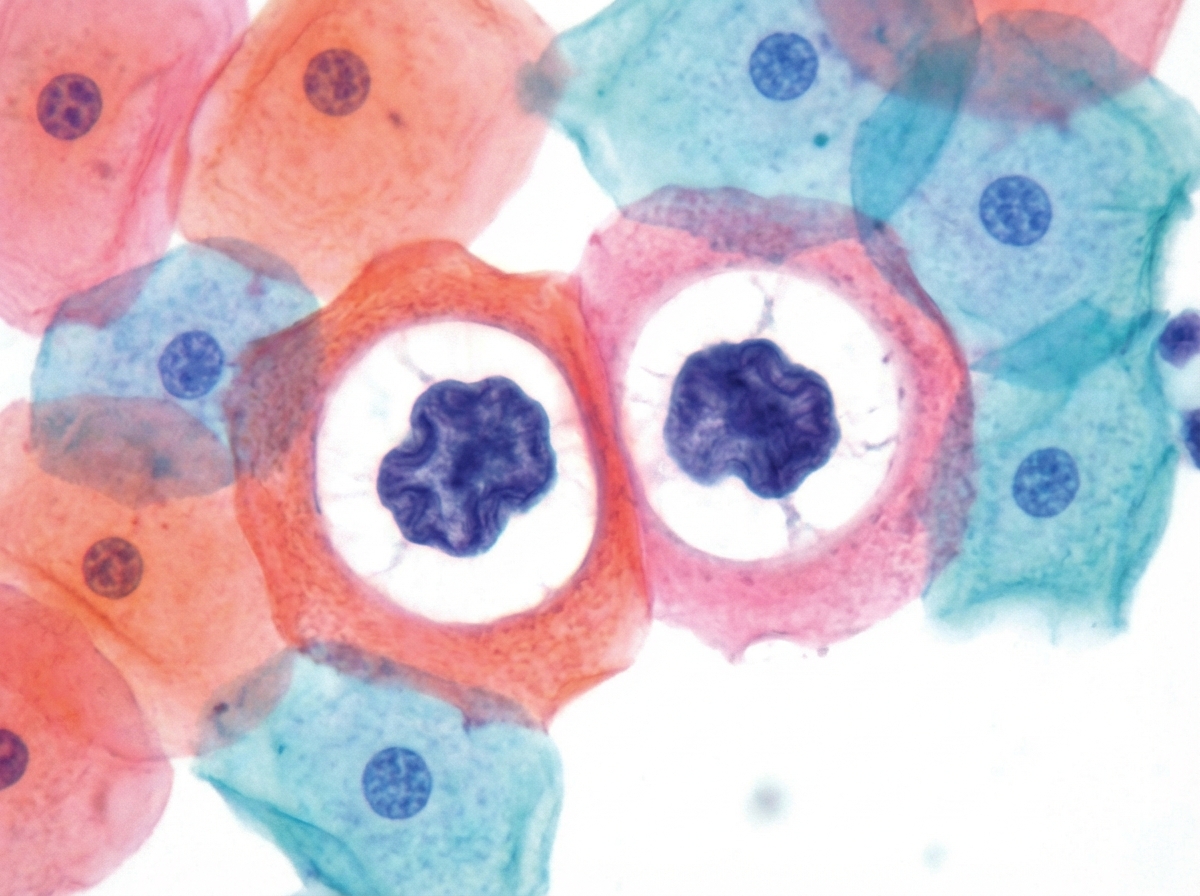
A 31-year-old woman presents to her gynecologist for a routine well-visit. She is sexually active with multiple male partners and uses an intrauterine device for contraception. Her last menstrual period was two weeks ago. She denies abnormal vaginal discharge or sensations of burning or itching. Pelvic exam is normal. Routine Pap smear shows the following (see Image A). Which organism is most likely responsible for her abnormal Pap smear?
A 62-year-old man comes to the physician because of a growth on his penis that has been gradually increasing in size over the last year. He was diagnosed with HIV 10 years ago. He has been divorced for 25 years and has had “at least 30 sexual partners” since. Physical examination shows a nontender 2.5-cm ulcerated lesion with an erythematous base on the dorsum of the glans. There is firm left inguinal lymphadenopathy. A biopsy of the lesion shows small uniform basophilic cells with central necrosis that invade into the corpus cavernosum. This patient's condition is most likely associated with which of the following pathogens?
A 57-year-old man presents to the office with complaints of perianal pain during defecation and perineal heaviness for 1 month. He also complains of discharge around his anus, and bright red bleeding during defecation. The patient provides a history of having a sexual relationship with other men without using any methods of protection. The physical examination demonstrates edematous verrucous anal folds that are of hard consistency and painful to the touch. A proctosigmoidoscopy reveals an anal canal ulcer with well defined, indurated borders on a white background. A biopsy is taken and the results are pending. What is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app