
Oncogenic viruses — MCQs

On this page
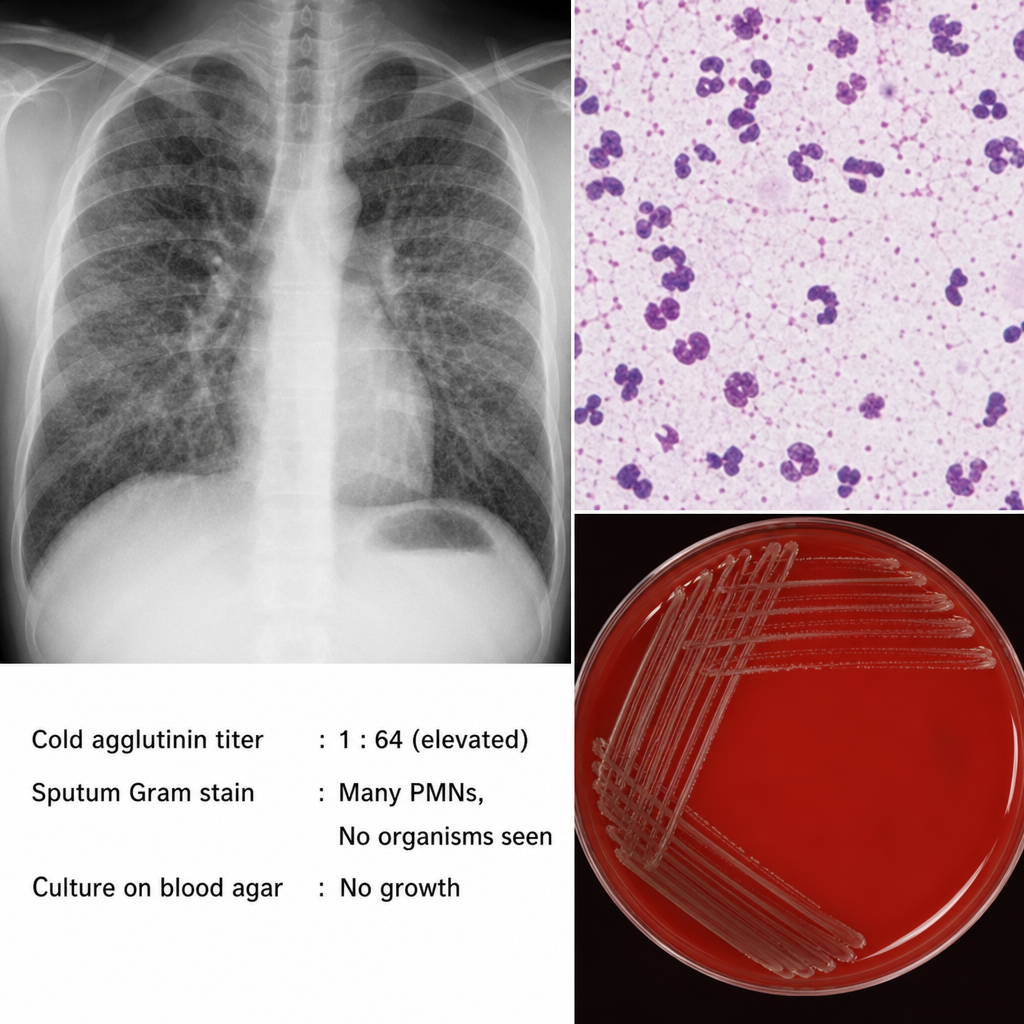
A 19-year-old college student presents with a 10-day history of low-grade fever, malaise, and a non-productive cough that has worsened despite a 5-day course of amoxicillin prescribed by his primary care physician. He lives in a dormitory. Chest radiograph shows diffuse interstitial infiltrates disproportionate to his relatively mild clinical appearance. A cold agglutinin titer is elevated. Sputum Gram stain shows many polymorphonuclear cells but no organisms. Cultures on standard blood agar show no growth after 48 hours. Which of the following features of the causative organism most directly explains the failure of amoxicillin therapy and the absence of organisms on Gram stain?
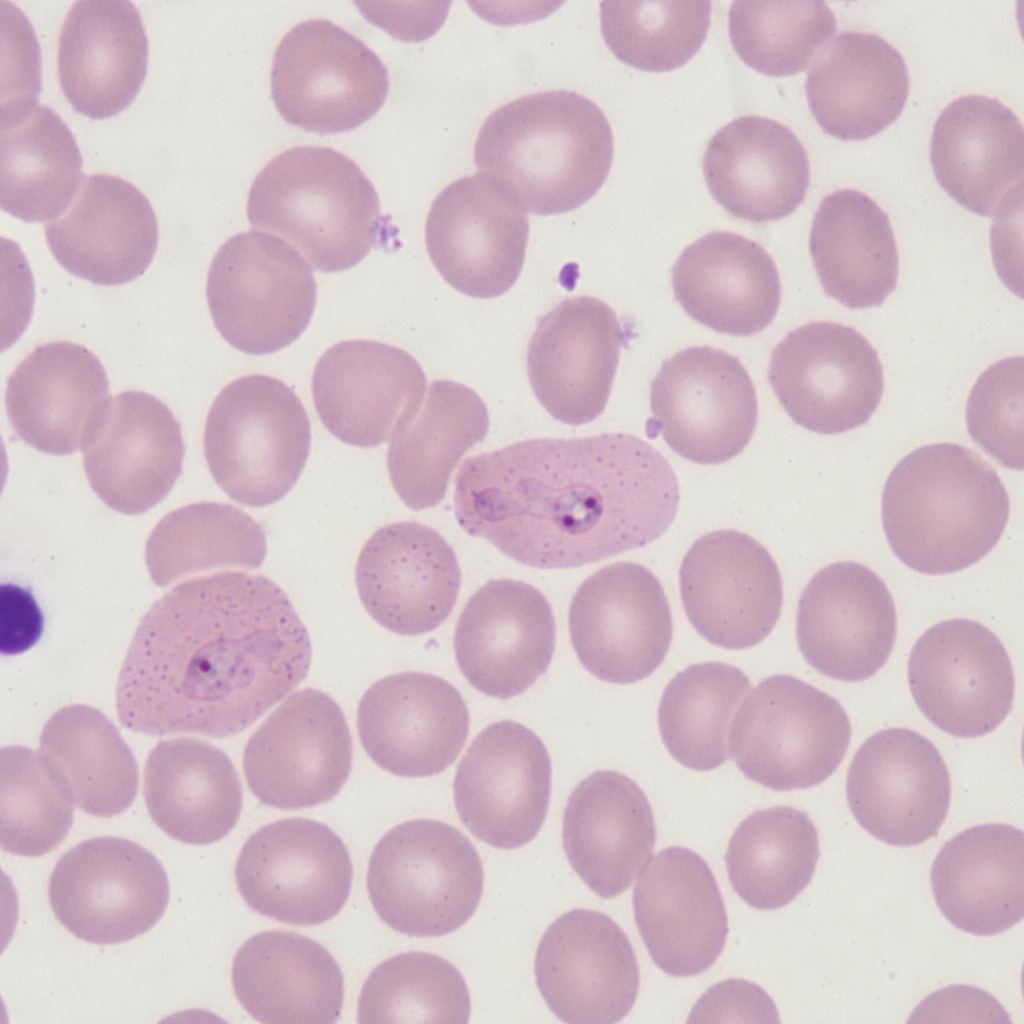
A blood smear from a 28-year-old traveler returning from South Asia shows enlarged erythrocytes with irregular, ameboid-appearing trophozoites and fine pink stippling of the red cell cytoplasm. The patient has a fever every 48 hours and hemoglobin of 11.8 g/dL. Which of the following morphological features on this smear most specifically distinguishes the causative organism from other species in the same genus?
A 16-year-old male is brought to the clinic by his mother for the complaints of fever, nonproductive cough, fatigue, lack of appetite, and sore throat for the past 2 months. Several other students at his high school have had similar symptoms. Physical exam shows a whitish membrane in his oropharynx, bilateral enlarged cervical lymphadenopathy, and mild splenomegaly. Which of the following tests is most likely to diagnose his condition?
A 55-year-old Caucasian male presents for a routine colonoscopy. A polyp is found in the patient's transverse colon and is found to be cancerous on histological evaluation. Upon examination, it is found that these cancerous cells have decreased MHC class I expression on their surface. Which immune system cell is most capable of killing these tumor cells?
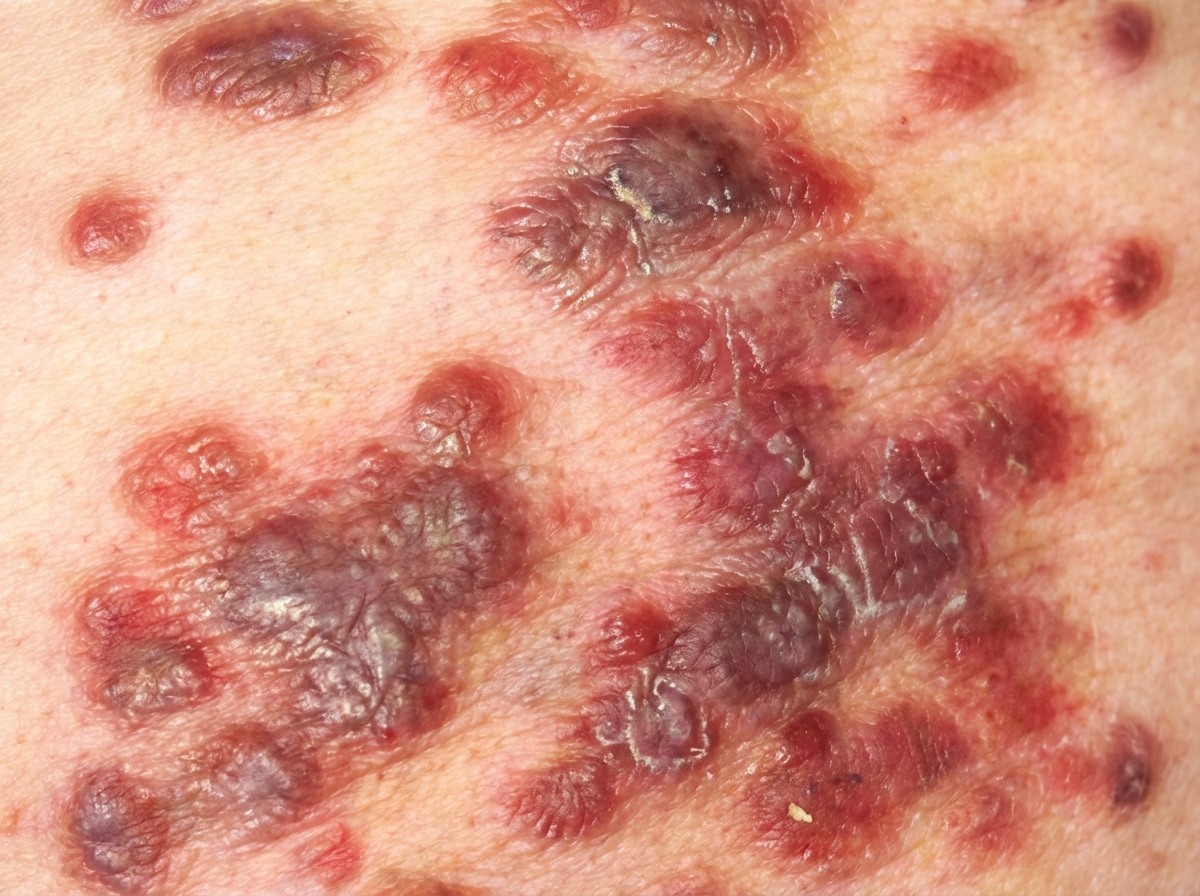
A 52-year-old woman presents to a local hospital complaining about a rash on her face and torso, as well as night sweats, low-grade fever, diarrhea, and unintentional weight loss. Her personal history is relevant for homelessness; she also has a history of risky behaviors such as the use and abuse of intravenous drugs, and unprotected intercourse with multiple sexual partners. Upon physical examination, well-demarcated violaceous plaques and papules distributed on her face and back are visible (see image below). Additional findings include fine reticular and interstitial changes on a chest radiograph, a CD4+ count of 50 cells/mm3, and positive HIV serology. Which of the following is the most likely etiology of this patient's dermatological condition?
A 28-year-old male with a history of HIV infection is found to have a CD4+ T lymphocyte count of 68 cells per microliter. As a consequence of his HIV infection, this patient is at increased risk of malignancy due to which of the following?
A scientist is researching the long term effects of the hepatitis viruses on hepatic tissue. She finds that certain strains are oncogenic and increase the risk of hepatocellular carcinoma. However, they appear to do so via different mechanisms. Which of the following answer choices correctly pairs the hepatitis virus with the correct oncogenic process?
A 48-year-old man comes to the physician because of a skin lesion on his nose and in his mouth. The lesions have been gradually increasing in size and are not painful or pruritic. Two months ago, he was treated for esophageal candidiasis. Physical examination shows one pinkish-brown papule on the right wing of the nose and two similar nodular lesions on the hard palate and buccal mucosa. A biopsy of one of the lesions shows spindle-shaped endothelial cells and infiltration of lymphocytes, plasma cells, and macrophages. Which of the following is the most likely causal organism of this patient's condition?
A 42-year-old man presents with an oral cavity lesion, toothache, and weight loss. He is known to have been HIV-positive for 6 years, but he does not follow a prescribed antiretroviral regimen because of personal beliefs. The vital signs are as follows: blood pressure 110/80 mm Hg, heart rate 89/min, respiratory rate 17/min, and temperature 37.1°C (100.8°F). The physical examination revealed an ulcerative lesion located on the lower lip. The lesion was friable, as evidenced by contact bleeding, and tender on palpation. A CT scan showed the lesion to be a solid mass (7 x 6 x 7 cm3) invading the mandible and spreading to the soft tissues of the oral cavity floor. A biopsy was obtained to determine the tumor type, which showed a monotonous diffuse lymphoid proliferation of large cells with plasmablastic differentiation, and oval-to-round vesicular nuclei with fine chromatin. The cells are immunopositive for VS38c. DNA of which of the following viruses is most likely to be identified in the tumor cells?
A 36-year-old woman comes to the physician because of growths around her anus that developed over the past 4 weeks. They are not painful and she does not have blood in her stool. She is sexually active with two male partners and uses condoms inconsistently. She appears healthy. Vital signs are within normal limits. Examination shows nontender, irregular, hyperkeratotic sessile lesions in the perianal area around 4–7 mm in diameter. There is no lymphadenopathy. The application of a dilute solution of acetic acid turns the lesions white. Which of the following is the most likely cause of the lesions?
Practice by Chapter
Human papillomavirus
Practice Questions
HPV-associated cancers
Practice Questions
HPV vaccination and screening
Practice Questions
Epstein-Barr virus
Practice Questions
EBV-associated malignancies
Practice Questions
Hepatitis B and hepatocellular carcinoma
Practice Questions
Hepatitis C and hepatocellular carcinoma
Practice Questions
Human T-cell leukemia virus
Practice Questions
Merkel cell polyomavirus
Practice Questions
Human herpesvirus 8 (Kaposi sarcoma virus)
Practice Questions
Mechanisms of viral oncogenesis
Practice Questions
Cancer prevention strategies for oncogenic viruses
Practice Questions
Therapeutic approaches targeting oncogenic viruses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app