
Skin microbiome — MCQs

A 21-year-old man comes to the physician because of painful, firm, dark bumps on his neck and jawline. He has no history of serious illness and takes no medications. His brother had a similar rash. A photograph of the rash is shown. Which of the following is the most likely underlying mechanism of this patient's condition?

A 65-year-old man presents to the emergency department with a complaint of intense pain in his right foot for the past month, along with fever and chills. He denies any traumatic injury to his foot in recent memory. He has a medical history of poorly-controlled type II diabetes and is a former smoker with extensive peripheral vascular disease. On physical exam, the area of his right foot around the hallux is swollen, erythematous, tender to light palpation, and reveals exposed bone. Labs are notable for elevated C-reactive protein and erythrocyte sedimentation rate. The physician obtains a biopsy for culture. What is the most likely causative organism for this patient’s condition?
A 47-year-old woman comes to the physician because of a 6-week history of fatigue and low-grade fever. She has no history of serious illness except for a bicuspid aortic valve, diagnosed 10 years ago. She does not use illicit drugs. Her temperature is 37.7°C (99.9°F). Physical examination shows petechiae under the fingernails and multiple tender, red nodules on the fingers. A new grade 2/6 diastolic murmur is heard at the right second intercostal space. Which of the following is the most likely causal organism?
A 65-year-old woman undergoes an abdominal hysterectomy. She develops pain and discharge at the incision site on the fourth postoperative day. The past medical history is significant for diabetes of 12 years duration, which is well-controlled on insulin. Pus from the incision site is sent for culture on MacConkey agar, which shows white-colorless colonies. On blood agar, the colonies were green. Biochemical tests reveal an oxidase-positive organism. Which of the following is the most likely pathogen?
A 63-year-old female recovering from a total shoulder arthroplasty completed 6 days ago presents complaining of joint pain in her repaired shoulder. Temperature is 39 degrees Celsius. Physical examination demonstrates erythema and significant tenderness around the incision site. Wound cultures reveal Gram-positive cocci that are resistant to nafcillin. Which of the following organisms is the most likely cause of this patient's condition?
Blood cultures are sent to the laboratory. Intravenous antibiotic therapy is started. Transesophageal echocardiography shows a large, oscillating vegetation attached to the tricuspid valve. There are multiple small vegetations attached to tips of the tricuspid valve leaflets. There is moderate tricuspid regurgitation. The left side of the heart and the ejection fraction are normal. Which of the following is the most likely causal organism of this patient's condition?
A 27-year-old female presents to her primary care physician because she is concerned about lighter colored patches on her skin. She recently went sunbathing and noticed that these areas also did not tan. Her doctor explains that she has a fungal infection of the skin that damages melanocytes by producing acids. She is prescribed selenium sulfide and told to follow-up in one month. Which of the following describes the appearance of the most likely infectious organism under microscopy?
A 36-year-old man comes to the physician because of a 2-day history of malaise and a painful, pruritic rash on his lower back and thighs. His temperature is 37.8°C (100°F). Physical examination shows the findings in the photograph. Skin scrapings from the thigh grow neutral colonies on MacConkey agar. The colony-producing bacteria are oxidase-positive. Which of the following is the greatest risk factor for the patient's condition?

A 24-year-old man presents with low-grade fever and shortness of breath for the last 3 weeks. Past medical history is significant for severe mitral regurgitation status post mitral valve replacement five years ago. His temperature is 38.3°C (101.0°F) and respiratory rate is 18/min. Physical examination reveals vertical hemorrhages under his nails, multiple painless erythematous lesions on his palms, and two tender, raised nodules on his fingers. Cardiac auscultation reveals a new-onset 2/6 holosystolic murmur loudest at the apex with the patient in the left lateral decubitus position. A transesophageal echocardiogram reveals vegetations on the prosthetic valve. Blood cultures reveal catalase-positive, gram-positive cocci. Which of the following characteristics is associated with the organism most likely responsible for this patient’s condition?
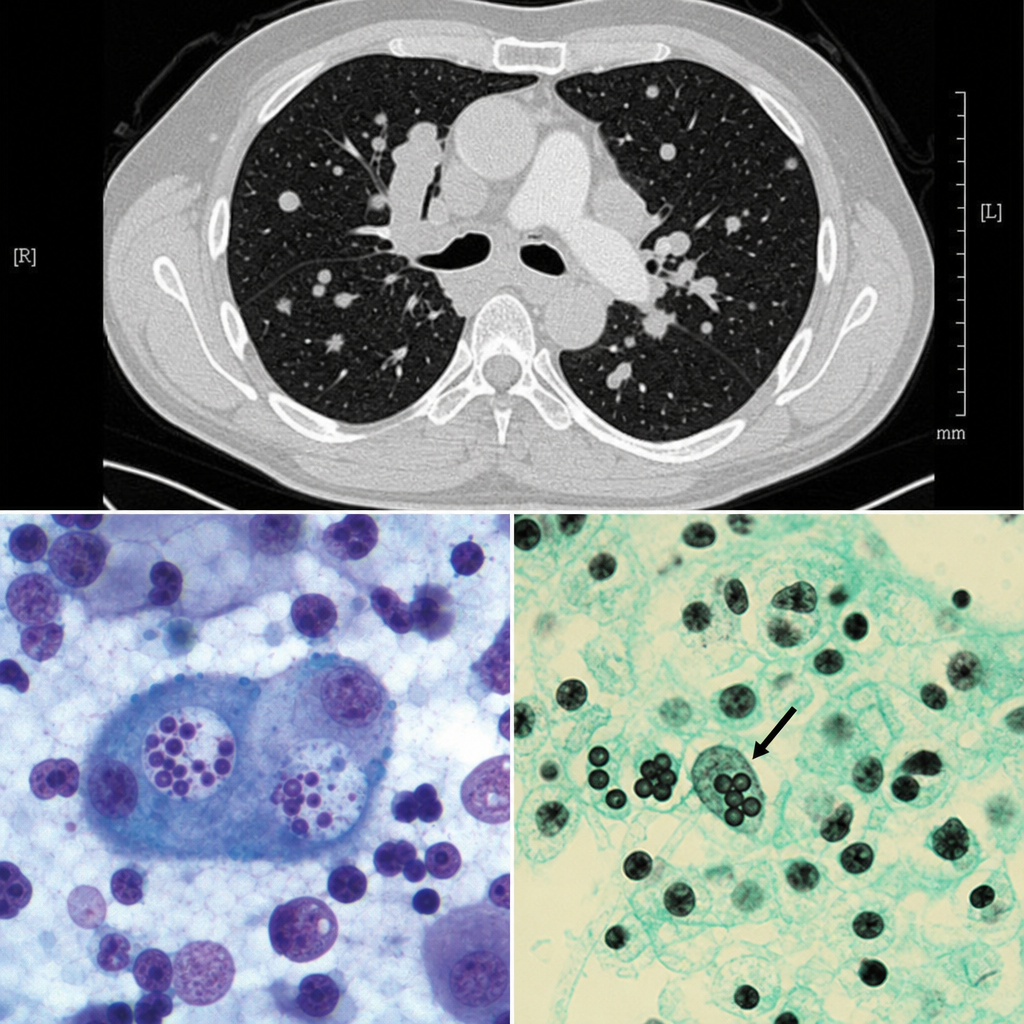
A 38-year-old man from the Mississippi River Valley presents with a 3-week history of fever, night sweats, and weight loss. He works as a cave explorer. Chest CT shows mediastinal lymphadenopathy and multiple pulmonary nodules. Bronchoalveolar lavage is performed and a silver stain of the specimen reveals small (2–4 µm) oval yeast forms within the cytoplasm of alveolar macrophages. Cultures at 25°C grow a mold with tuberculate macroconidia. Which of the following correctly describes the tissue form of this organism and its mechanism of immune evasion?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app