
Respiratory tract microbiome — MCQs

A 12-year-old boy presents to the emergency room with difficulty breathing after several days of severe sore throat. Further history reveals that his family immigrated recently from Eastern Europe and he has never previously seen a doctor. Physical exam shows cervical lymphadenopathy with extensive neck edema as well as the finding shown in the image provided. You suspect a bacteria that causes the disease by producing an AB type exotoxin. Which of the following is the proper medium to culture the most likely cause of this infection?

A 63-year-old man comes to the physician for evaluation of fever and a nonproductive cough for the past 2 weeks. During this period, he has also had fatigue, myalgia, and difficulty breathing. Five weeks ago, he underwent an aortic prosthetic valve replacement due to high-grade aortic stenosis. The patient has a history of hypertension, asthma, and type 2 diabetes mellitus. A colonoscopy 2 years ago was normal. The patient has smoked one pack of cigarettes daily for the past 40 years. He has never used illicit drugs. Current medications include aspirin, warfarin, lisinopril, metformin, inhaled albuterol, and a multivitamin. The patient appears lethargic. Temperature is 38.6°C (101.5°F), pulse is 105/min, and blood pressure is 140/60 mm Hg. Rales are heard on auscultation of the lungs. A grade 2/6, diastolic blowing murmur is heard over the left sternal border and radiates to the right sternal border. A photograph of his right index finger is shown. Laboratory studies show a leukocyte count of 13,800/mm3 and an erythrocyte sedimentation rate of 48 mm/h. Which of the following is the most likely causal organism?

An investigator is studying the growth of an organism in different media. The organism is inoculated on a petri dish that contains heated sheep blood, vancomycin, nystatin, trimethoprim, and colistin. The resulting growth medium is incubated at 37°C. Numerous small, white colonies are seen after incubation for 48 hours. This organism is most likely to cause which of the following conditions?
A 40-year-old man presents to the office complaining of chills, fever, and productive cough for the past 24 hours. He has a history of smoking since he was 18 years old. His vitals are: heart rate of 85/min, respiratory rate of 20/min, temperature 39.0°C (102.2°F), blood pressure 110/70 mm Hg. On physical examination, there is dullness on percussion on the upper right lobe, as well as bronchial breath sounds and egophony. The plain radiograph reveals an increase in density with an alveolar pattern in the upper right lobe. Which one is the most common etiologic agent of the suspected disease?
A patient is hospitalized for pneumonia. Gram-positive cocci in clusters are seen on sputum gram stain. Which of the following clinical scenarios is most commonly associated with this form of pneumonia?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
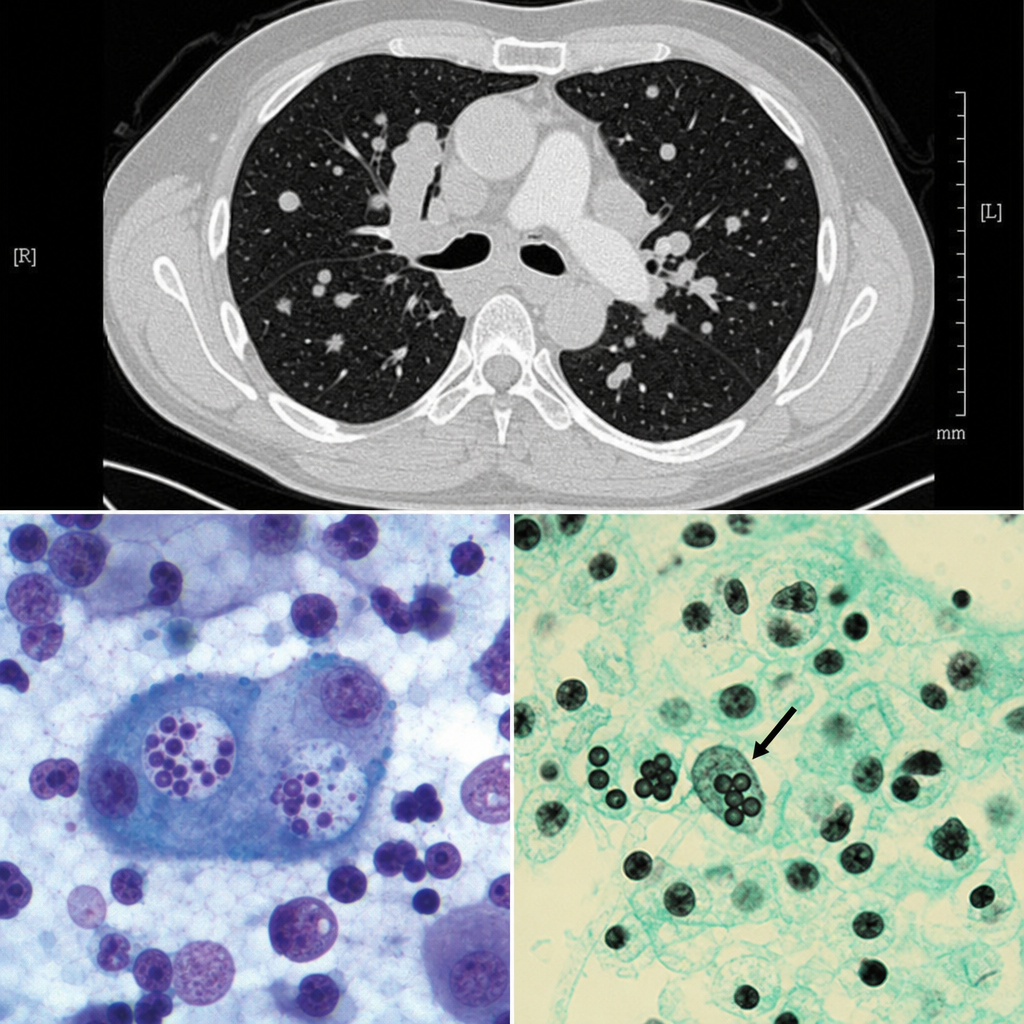
A 35-year-old man comes to the emergency department with fever, chills, dyspnea, and a productive cough. His symptoms began suddenly 2 days ago. He was diagnosed with HIV 4 years ago and has been on triple antiretroviral therapy since then. He smokes one pack of cigarettes daily. He is 181 cm (5 ft 11 in) tall and weighs 70 kg (154 lb); BMI is 21.4 kg/m2. He lives in Illinois and works as a carpenter. His temperature is 38.8°C (101.8°F), pulse is 110/min, respirations are 24/min, and blood pressure is 105/74 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 92%. Examinations reveals crackles over the right lower lung base. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 11.5 g/dL Leukocyte count 12,800/mm3 Segmented neutrophils 80% Eosinophils 1% Lymphocytes 17% Monocytes 2% CD4+ T-lymphocytes 520/mm3(N ≥ 500) Platelet count 258,000/mm3 Serum Na+ 137 mEq/L Cl- 102 mEq/L K+ 5.0 mEq/L HCO3- 22 mEq/L Glucose 92 mg/dL An x-ray of the chest shows a right lower-lobe infiltrate of the lung. Which of the following is the most likely causal organism?
While testing various strains of Streptococcus pneumoniae, a researcher discovers that a certain strain of this bacteria is unable to cause disease in mice when deposited in their lungs. What physiological test would most likely deviate from normal in this strain of bacteria as opposed to a typical strain?
A 46-year-old woman presents to her primary care physician with complaints of increasing left upper quadrant discomfort. She has a known history of type 1 Gaucher disease. On physical examination, her spleen is palpable 8 cm below the costal margin. Routine laboratory work reveals severe pancytopenia. After consultation with the patient on the risks of her condition, the patient decides to undergo a splenectomy. Which of the following is more likely to occur as a consequence of splenectomy in this patient?
A 38-year-old man from the Mississippi River Valley presents with a 3-week history of fever, night sweats, and weight loss. He works as a cave explorer. Chest CT shows mediastinal lymphadenopathy and multiple pulmonary nodules. Bronchoalveolar lavage is performed and a silver stain of the specimen reveals small (2–4 µm) oval yeast forms within the cytoplasm of alveolar macrophages. Cultures at 25°C grow a mold with tuberculate macroconidia. Which of the following correctly describes the tissue form of this organism and its mechanism of immune evasion?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app