
Fecal microbiota transplantation — MCQs

A 72-year-old woman presents to the clinic complaining of diarrhea for the past week. She mentions intense fatigue and intermittent, cramping abdominal pain. She has not noticed any blood in her stool. She recalls an episode of pneumonia last month for which she was hospitalized and treated with antibiotics. She has traveled recently to Florida to visit her family and friends. Her past medical history is significant for hypertension, peptic ulcer disease, and hypercholesterolemia for which she takes losartan, esomeprazole, and atorvastatin. She also has osteoporosis, for which she takes calcium and vitamin D and occasional constipation for which she takes an over the counter laxative as needed. Physical examination shows lower abdominal tenderness but is otherwise insignificant. Blood pressure is 110/70 mm Hg, pulse is 80/min, and respiratory rate is 18/min. Stool testing is performed and reveals the presence of anaerobic, gram-positive bacilli. Which of the following increased this patient’s risk of developing this clinical presentation?
A scientist is studying the mechanisms by which bacteria become resistant to antibiotics. She begins by obtaining a culture of vancomycin-resistant Enterococcus faecalis and conducts replicate plating experiments. In these experiments, colonies are inoculated onto a membrane and smeared on 2 separate plates, 1 containing vancomycin and the other with no antibiotics. She finds that all of the bacterial colonies are vancomycin resistant because they grow on both plates. She then maintains the bacteria in liquid culture without vancomycin while she performs her other studies. Fifteen generations of bacteria later, she conducts replicate plating experiments again and finds that 20% of the colonies are now sensitive to vancomycin. Which of the following mechanisms is the most likely explanation for why these colonies have become vancomycin sensitive?
A 42-year-old man with hypertension and type 2 diabetes mellitus is admitted to the hospital because of swelling and redness of the left leg for 3 days. He has chills and malaise. He is treated with intravenous clindamycin for 7 days. On the 8th day at the hospital, he has profuse, foul-smelling, and watery diarrhea. He has nausea and intermittent abdominal cramping. His temperature is 38°C (100.4°F), pulse is 97/min, and blood pressure is 110/78 mm Hg. Bowel sounds are hyperactive. Abdominal examination shows mild tenderness in the left lower quadrant. Rectal examination shows no abnormalities. His hemoglobin concentration is 14.3 g/dL, leukocyte count is 12,300/mm3, and C-reactive protein concentration is 62 mg/L (N=0.08–3.1). After discontinuing clindamycin, which of the following is the most appropriate pharmacotherapy for this patient's condition?
A 21-year-old woman comes to the physician because of a 4-day history of abdominal cramps and bloody diarrhea 5 times per day. Her symptoms began after she ate an egg sandwich from a restaurant. Her vital signs are within normal limits. Physical examination shows diffuse abdominal tenderness. Stool culture shows gram-negative rods that produce hydrogen sulfide and do not ferment lactose. Which of the following effects is most likely to occur if she receives antibiotic therapy?
A 58-year-old female, being treated on the medical floor for community-acquired pneumonia with levofloxacin, develops watery diarrhea. She reports at least 9 episodes of diarrhea within the last two days, with lower abdominal discomfort and cramping. Her temperature is 98.6° F (37° C), respiratory rate is 15/min, pulse is 67/min, and blood pressure is 122/98 mm Hg. Her physical examination is unremarkable. Laboratory testing shows: Hb% 13 gm/dL Total count (WBC): 13,400/mm3 Differential count: Neutrophils: 80% Lymphocytes: 15% Monocytes: 5% ESR: 33 mm/hr What is the most likely diagnosis?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 54-year-old man presents with fever, abdominal pain, nausea, and bloody diarrhea. He says that his symptoms started 36 hours ago and have not improved. Past medical history is significant for a left-leg abscess secondary to an injury he sustained from a fall 4 days ago while walking his dog. He has been taking clindamycin for this infection. In addition, he has long-standing gastroesophageal reflux disease, managed with omeprazole. His vital signs include: temperature 38.5°C (101.3°F), respiratory rate 19/min, heart rate 90/min, and blood pressure 110/70 mm Hg. Which of the following is the best course of treatment for this patient’s most likely diagnosis?
A 49-year-old man presents to the emergency department with acute onset of pain and redness of the skin of his lower leg for the past 3 days. He has had type 2 diabetes mellitus for the past 12 years, but he is not compliant with his medications. He has smoked 10–15 cigarettes per day for the past 20 years. His temperature is 38°C (100.4°F), pulse is 95/min, and blood pressure is 110/70 mm Hg. On physical examination, the pretibial area is erythematous, edematous, and tender. He is diagnosed with acute cellulitis, and intravenous ceftazidime sodium is started. On the 5th day of antibiotic therapy, the patient complains of severe watery diarrhea, fever, and abdominal tenderness without rigidity. Complete blood count is ordered for the patient and shows 14,000 white blood cells/mm3. Which of the following is the best initial therapy for this patient?
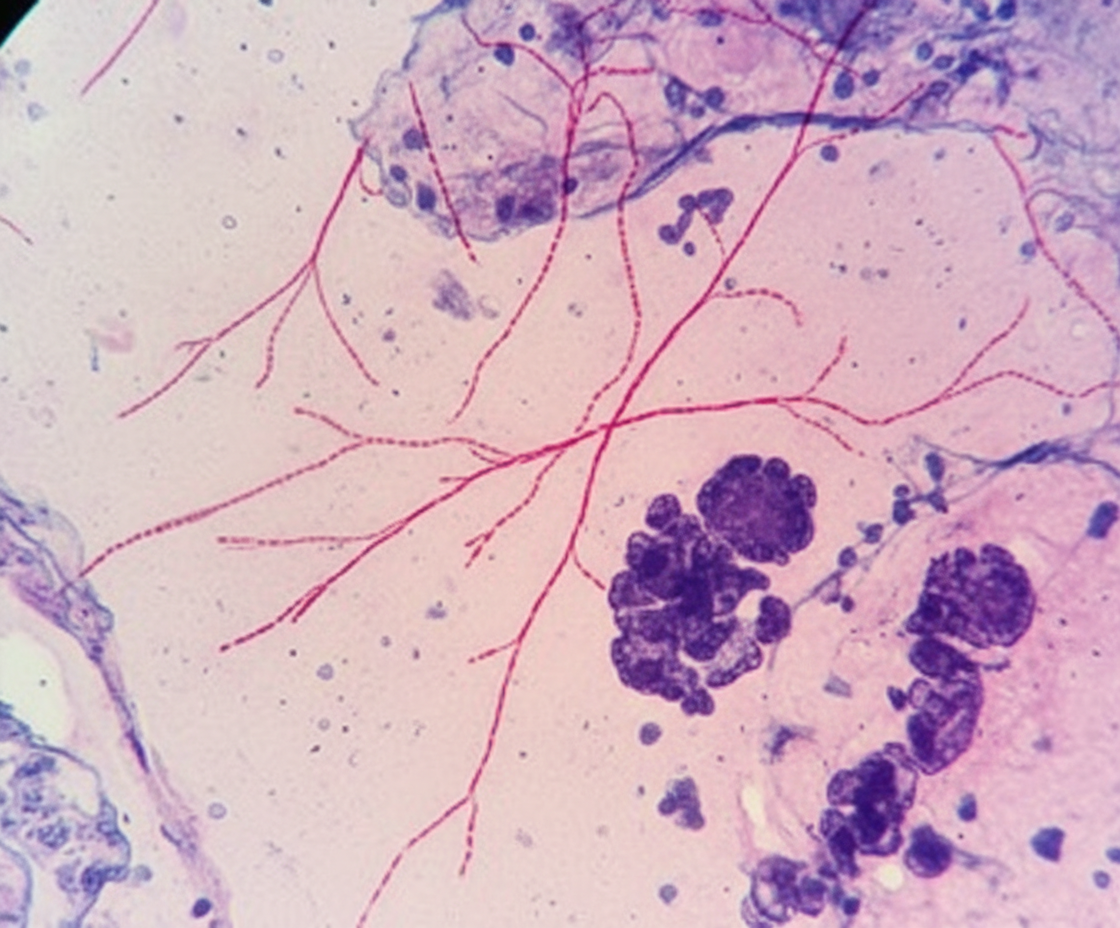
A 68-year-old man comes to the physician because of a 1-month history of fatigue, low-grade fevers, and cough productive of blood-tinged sputum. He has type 2 diabetes mellitus and chronic kidney disease and underwent kidney transplantation 8 months ago. His temperature is 38.9°C (102.1°F) and pulse is 98/min. Examination shows rhonchi in the right lower lung field. An x-ray of the chest shows a right-sided lobar consolidation. A photomicrograph of specialized acid-fast stained tissue from a blood culture is shown. Which of the following is the strongest predisposing factor for this patient's condition?
A 55-year-old man presents to the physician with complaints of 5 days of watery diarrhea, fever, and bloating. He has not noticed any blood in his stool. He states that his diet has not changed recently, and his family has been spared from diarrhea symptoms despite eating the same foods that he has been cooking at home. He has no history of recent travel outside the United States. His only medication is high-dose omeprazole, which he has been taking daily for the past few months to alleviate his gastroesophageal reflux disease (GERD). Which of the following is the most appropriate initial test to work up this patient’s symptoms?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app