
Dysbiosis and disease associations — MCQs

An investigator is studying the growth of an organism in different media. The organism is inoculated on a petri dish that contains heated sheep blood, vancomycin, nystatin, trimethoprim, and colistin. The resulting growth medium is incubated at 37°C. Numerous small, white colonies are seen after incubation for 48 hours. This organism is most likely to cause which of the following conditions?
A previously healthy 20-year-old woman comes to the physician because of recurrent abdominal cramps, bloating, and diarrhea for 4 months. She describes her stools as greasy, foul-smelling, and difficult to flush. During this time she has had a 6-kg (13.2-lb) weight loss. She has no personal or family history of serious illness. Physical examination shows pallor and cheilitis. Laboratory studies show a hemoglobin concentration of 11 g/dL. Serum concentrations of electrolytes, urea nitrogen, and creatinine are within the reference range. Test of the stool for occult blood is negative and stool microscopy reveals no pathogens and no leukocytes. Analysis of a 24-hour stool sample shows 12 g of fat. The patient is asked to consume 25 g of d-xylose. Five hours later, its concentration is measured in urine at 2 g (N = > 4 g/5 h). The test is repeated after a two-week course of rifaximin, but the urinary concentration of d-xylose remains the same. Which of the following is the most likely diagnosis?
A 57-year-old HIV-positive male with a history of intravenous drug abuse presents to the emergency room complaining of arm swelling. He reports that he developed progressively worsening swelling and tenderness over the right antecubital fossa three days prior. He recently returned from a trip to Nicaragua. His past medical history is notable for an anaphylactoid reaction to vancomycin. His temperature is 101.4°F (38.6°C), blood pressure is 140/70 mmHg, pulse is 110/min, and respirations are 20/min. Physical examination reveals an erythematous, fluctuant, and tender mass overlying the right antecubital fossa. Multiple injection marks are noted across both upper extremities. He undergoes incision and drainage and is started on an antibiotic that targets the 50S ribosome. He is discharged with plans to follow up in one week. However, five days later he presents to the same emergency room complaining of abdominal cramps and watery diarrhea. Which of the following classes of pathogens is most likely responsible for this patient’s current symptoms?
A 21-year-old woman comes to the physician because of a 4-day history of abdominal cramps and bloody diarrhea 5 times per day. Her symptoms began after she ate an egg sandwich from a restaurant. Her vital signs are within normal limits. Physical examination shows diffuse abdominal tenderness. Stool culture shows gram-negative rods that produce hydrogen sulfide and do not ferment lactose. Which of the following effects is most likely to occur if she receives antibiotic therapy?
A 55-year-old man presents to the physician with complaints of 5 days of watery diarrhea, fever, and bloating. He has not noticed any blood in his stool. He states that his diet has not changed recently, and his family has been spared from diarrhea symptoms despite eating the same foods that he has been cooking at home. He has no history of recent travel outside the United States. His only medication is high-dose omeprazole, which he has been taking daily for the past few months to alleviate his gastroesophageal reflux disease (GERD). Which of the following is the most appropriate initial test to work up this patient’s symptoms?
A 54-year-old man comes to the physician because of diarrhea that has become progressively worse over the past 4 months. He currently has 4–6 episodes of foul-smelling stools per day. Over the past 3 months, he has had fatigue and a 5-kg (11-lb) weight loss. He returned from Bangladesh 6 months ago after a year-long business assignment. He has osteoarthritis and hypertension. Current medications include amlodipine and naproxen. He appears pale and malnourished. His temperature is 37.3°C (99.1°F), pulse is 76/min, and blood pressure is 140/86 mm Hg. Examination shows pale conjunctivae and dry mucous membranes. Angular stomatitis and glossitis are present. The abdomen is distended but soft and nontender. Rectal examination shows no abnormalities. Laboratory studies show: Hemoglobin 8.9 g/dL Leukocyte count 4100/mm3 Platelet count 160,000/mm3 Mean corpuscular volume 110 μm3 Serum Na+ 133 mEq/L Cl- 98 mEq/l K+ 3.3 mEq/L Creatinine 1.1 mg/dL IgA 250 mg/dL Anti-tissue transglutaminase, IgA negative Stool culture and studies for ova and parasites are negative. Test of the stool for occult blood is negative. Fecal fat content is 22 g/day (N < 7). Fecal lactoferrin is negative and elastase is within normal limits. Which of the following is the most appropriate next step in diagnosis?
A 45-year-old man comes to the physician because of a 1-month history of fever and poor appetite. Five weeks ago, he underwent molar extraction for dental caries. His temperature is 38°C (100.4°F). Cardiac examination shows a grade 2/6 holosystolic murmur heard best at the apex. A blood culture shows gram-positive, catalase-negative cocci. Transesophageal echocardiography shows a small vegetation on the mitral valve with mild regurgitation. The causal organism most likely has which of the following characteristics?
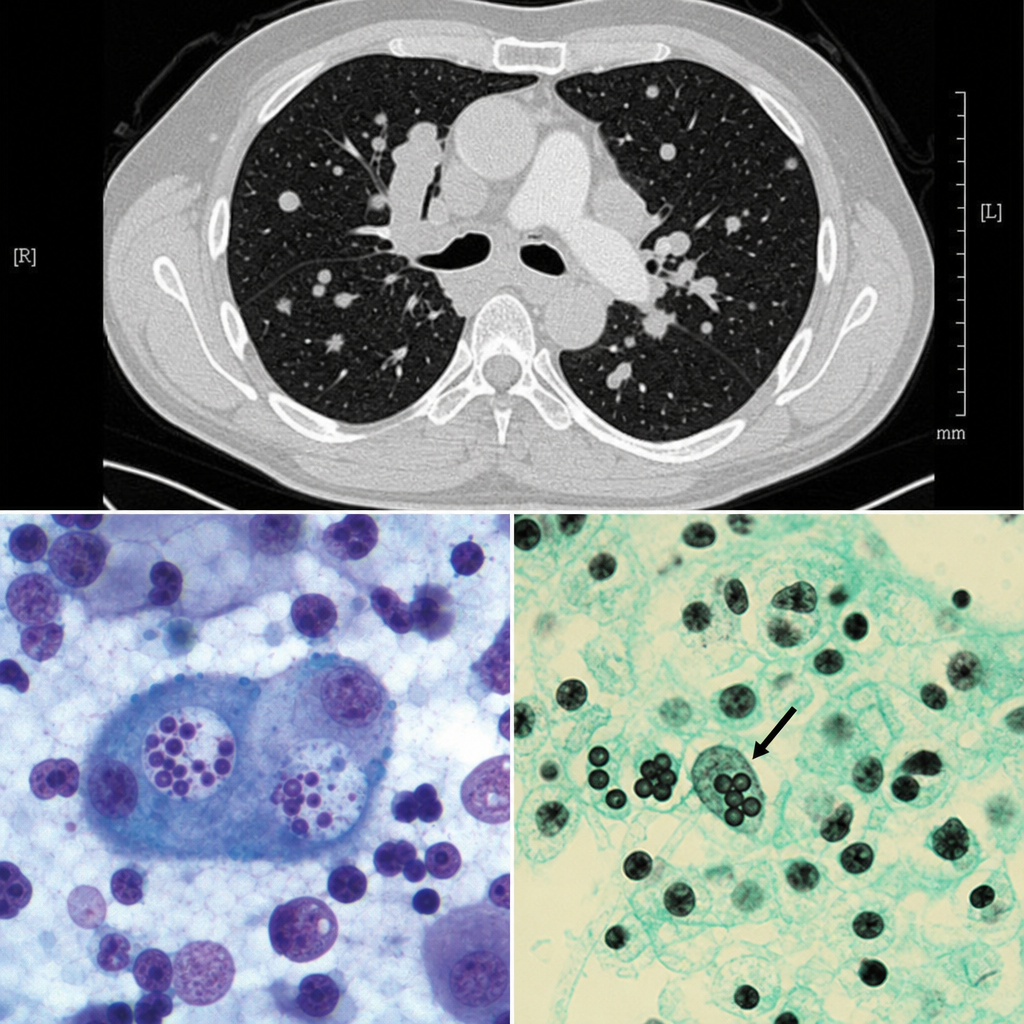
A 38-year-old man from the Mississippi River Valley presents with a 3-week history of fever, night sweats, and weight loss. He works as a cave explorer. Chest CT shows mediastinal lymphadenopathy and multiple pulmonary nodules. Bronchoalveolar lavage is performed and a silver stain of the specimen reveals small (2–4 µm) oval yeast forms within the cytoplasm of alveolar macrophages. Cultures at 25°C grow a mold with tuberculate macroconidia. Which of the following correctly describes the tissue form of this organism and its mechanism of immune evasion?
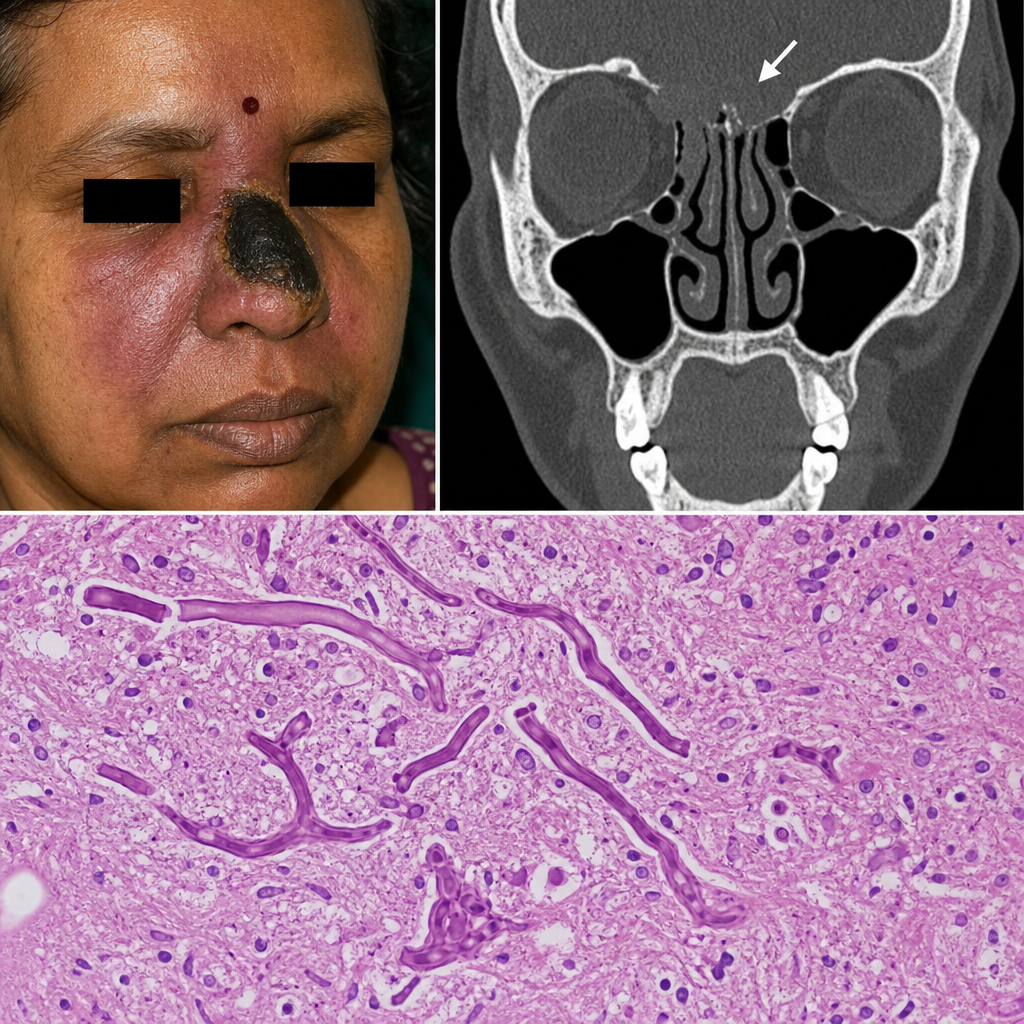
A 58-year-old woman with a history of poorly controlled type 2 diabetes is admitted with a 5-day history of fever, facial pain, and a black necrotic eschar over her right nasal bridge. CT imaging reveals bony erosion of the cribriform plate. A biopsy specimen is sent to the pathology laboratory. Which of the following best describes the expected histopathological findings?
A hospital implements a bundle to reduce catheter-associated bloodstream infections. Components include: chlorhexidine bathing, antibiotic-impregnated catheters, antiseptic catheter site dressings, and daily line necessity assessment. After implementation, bloodstream infections with coagulase-negative staphylococci decrease by 60%, but Candida bloodstream infections increase by 40%. Evaluate the microbiological mechanisms underlying these divergent outcomes and synthesize an optimal prevention strategy.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app