
Normal flora — MCQs

On this page
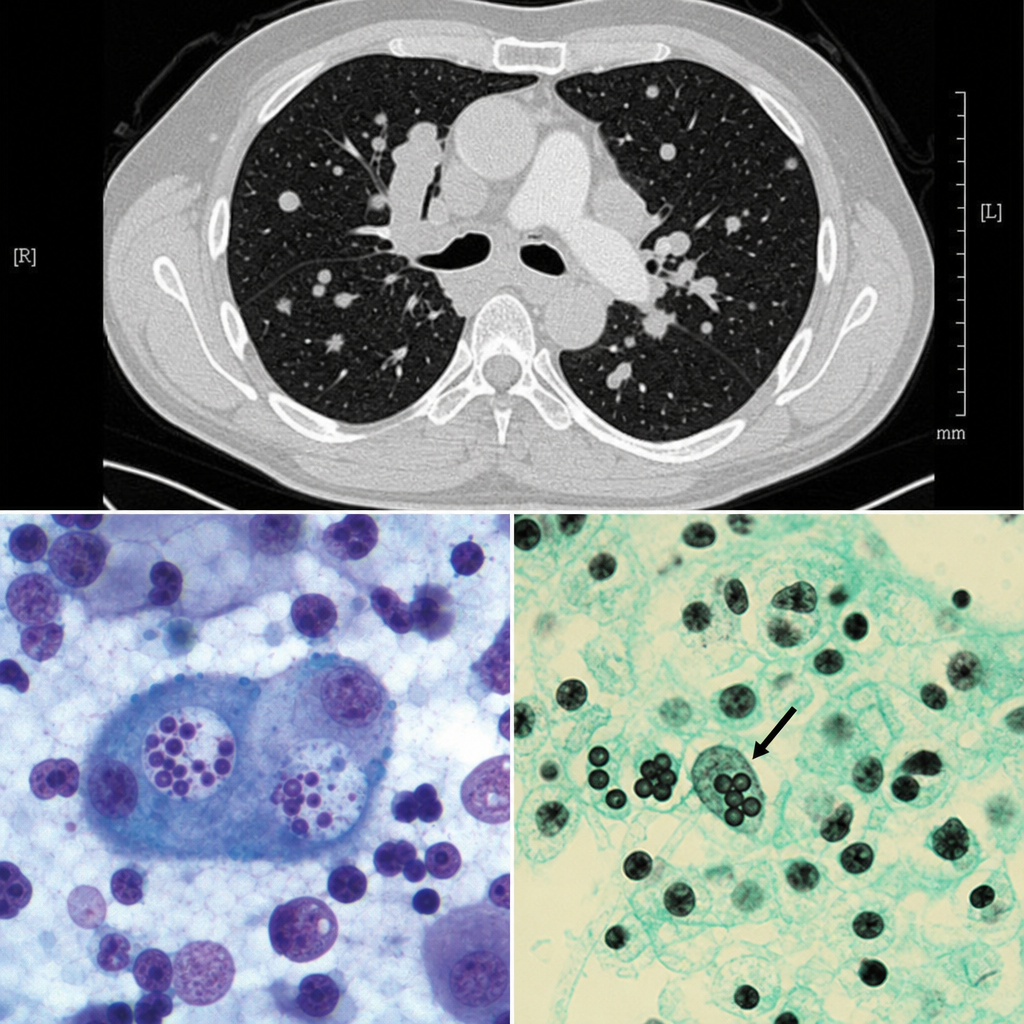
A 38-year-old man from the Mississippi River Valley presents with a 3-week history of fever, night sweats, and weight loss. He works as a cave explorer. Chest CT shows mediastinal lymphadenopathy and multiple pulmonary nodules. Bronchoalveolar lavage is performed and a silver stain of the specimen reveals small (2–4 µm) oval yeast forms within the cytoplasm of alveolar macrophages. Cultures at 25°C grow a mold with tuberculate macroconidia. Which of the following correctly describes the tissue form of this organism and its mechanism of immune evasion?
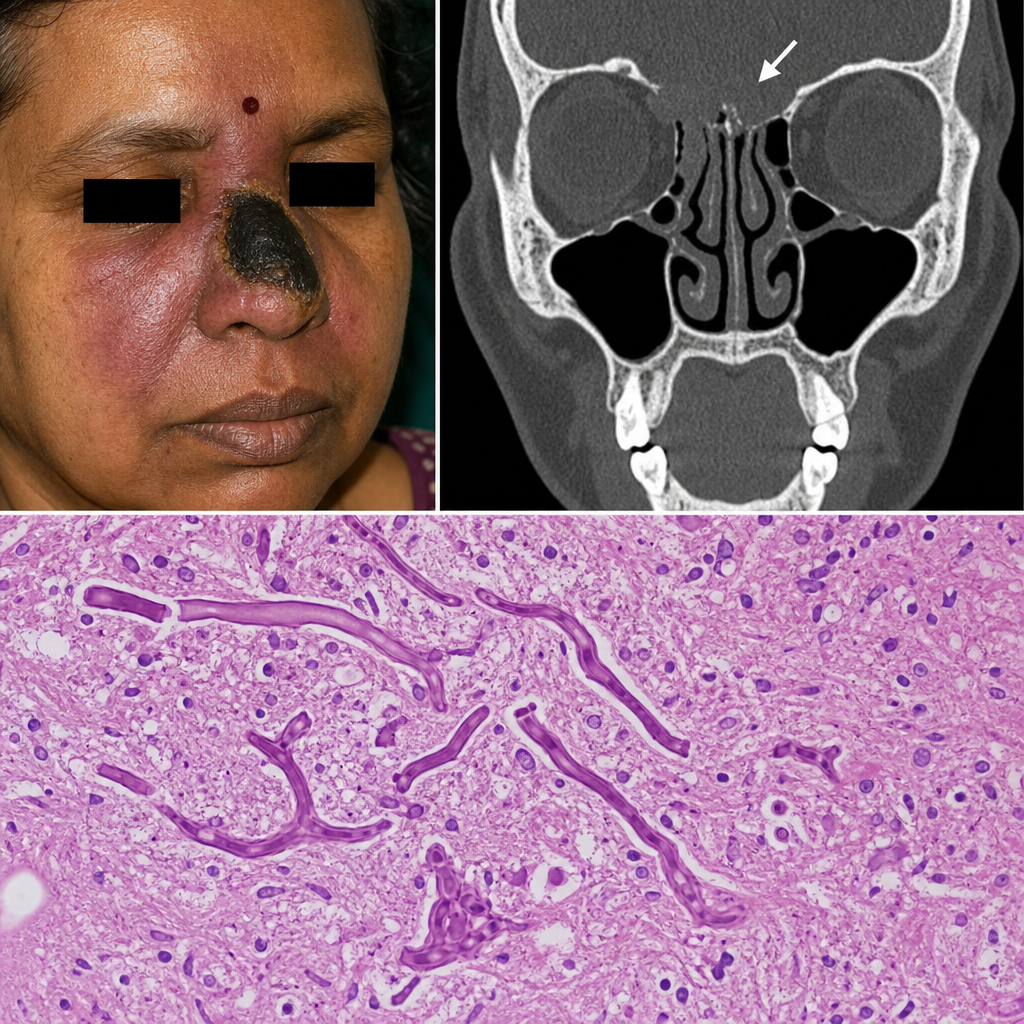
A 58-year-old woman with a history of poorly controlled type 2 diabetes is admitted with a 5-day history of fever, facial pain, and a black necrotic eschar over her right nasal bridge. CT imaging reveals bony erosion of the cribriform plate. A biopsy specimen is sent to the pathology laboratory. Which of the following best describes the expected histopathological findings?
A hospital implements a bundle to reduce catheter-associated bloodstream infections. Components include: chlorhexidine bathing, antibiotic-impregnated catheters, antiseptic catheter site dressings, and daily line necessity assessment. After implementation, bloodstream infections with coagulase-negative staphylococci decrease by 60%, but Candida bloodstream infections increase by 40%. Evaluate the microbiological mechanisms underlying these divergent outcomes and synthesize an optimal prevention strategy.
A 68-year-old man develops Clostridioides difficile infection after hospitalization for pneumonia. He is treated with oral vancomycin with resolution of diarrhea. Two weeks later, he has recurrent C. difficile infection. After a second vancomycin course, he has a third recurrence. His physician must choose between extended vancomycin taper, fidaxomicin, or fecal microbiota transplantation (FMT). Synthesize the microbiological rationale for selecting FMT over continued antibiotic therapy in recurrent C. difficile infection.
A research team is designing a probiotic intervention to prevent Clostridioides difficile infection in patients receiving antibiotics. They must choose between: (1) single-strain Lactobacillus; (2) multi-strain bacterial cocktail; (3) fecal microbiota transplantation; (4) prebiotic fiber supplementation. Evaluate which approach best applies principles of colonization resistance and normal flora restoration for PRIMARY prevention during antibiotic therapy.
A 32-year-old woman presents with malodorous vaginal discharge and vaginal pH of 5.5. Microscopy shows clue cells and a paucity of lactobacilli. She has been sexually active with a new partner for 2 months. Metronidazole treatment resolves her symptoms. Three months later, she returns with recurrent symptoms. Her partner is asymptomatic. Analyze the microbiological basis for treatment failure and the role of normal vaginal flora in this condition.
A 55-year-old man with cirrhosis and ascites undergoes diagnostic paracentesis. Fluid analysis shows 380 neutrophils/μL and culture grows Escherichia coli (single organism). He denies abdominal pain or fever. His primary care physician treated him with ciprofloxacin for a UTI one week ago. Analyze the most likely pathogenesis of this finding considering the role of normal flora and his recent antibiotic use.
A 3-month-old infant born prematurely at 28 weeks gestation is hospitalized in the NICU. She has been on broad-spectrum antibiotics for suspected sepsis and is receiving total parenteral nutrition. She develops abdominal distension, bloody stools, and pneumatosis intestinalis on X-ray. Blood cultures grow Clostridium perfringens. Analyze the relationship between her clinical course and alterations in intestinal flora that led to this condition.
A 62-year-old woman with a mechanical heart valve presents with fever and a new heart murmur. Blood cultures grow Streptococcus mutans. She reports having a dental cleaning 2 weeks prior without antibiotic prophylaxis. Her dentist states that current guidelines do not recommend prophylaxis for routine cleanings in most patients. Apply your knowledge of normal oral flora to determine why this patient should have received prophylaxis.
A 45-year-old man with newly diagnosed acute myeloid leukemia receives induction chemotherapy. On day 7 of neutropenia (absolute neutrophil count 100/μL), he develops fever to 39.2°C (102.6°F). Blood cultures grow Candida albicans. Which alteration in normal flora defense mechanisms best explains his susceptibility to this fungal infection?
Practice by Chapter
Skin microbiome
Practice Questions
Oral microbiome
Practice Questions
Respiratory tract microbiome
Practice Questions
Gastrointestinal microbiome
Practice Questions
Urogenital microbiome
Practice Questions
Development of microbiome from birth
Practice Questions
Microbiome functions and host defense
Practice Questions
Dysbiosis and disease associations
Practice Questions
Probiotics and prebiotics
Practice Questions
Microbiome in antibiotic-associated diarrhea
Practice Questions
Fecal microbiota transplantation
Practice Questions
Methods for studying the microbiome
Practice Questions
Microbiome and immune system interactions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app