
Microbial genetics and drug resistance — MCQs

On this page
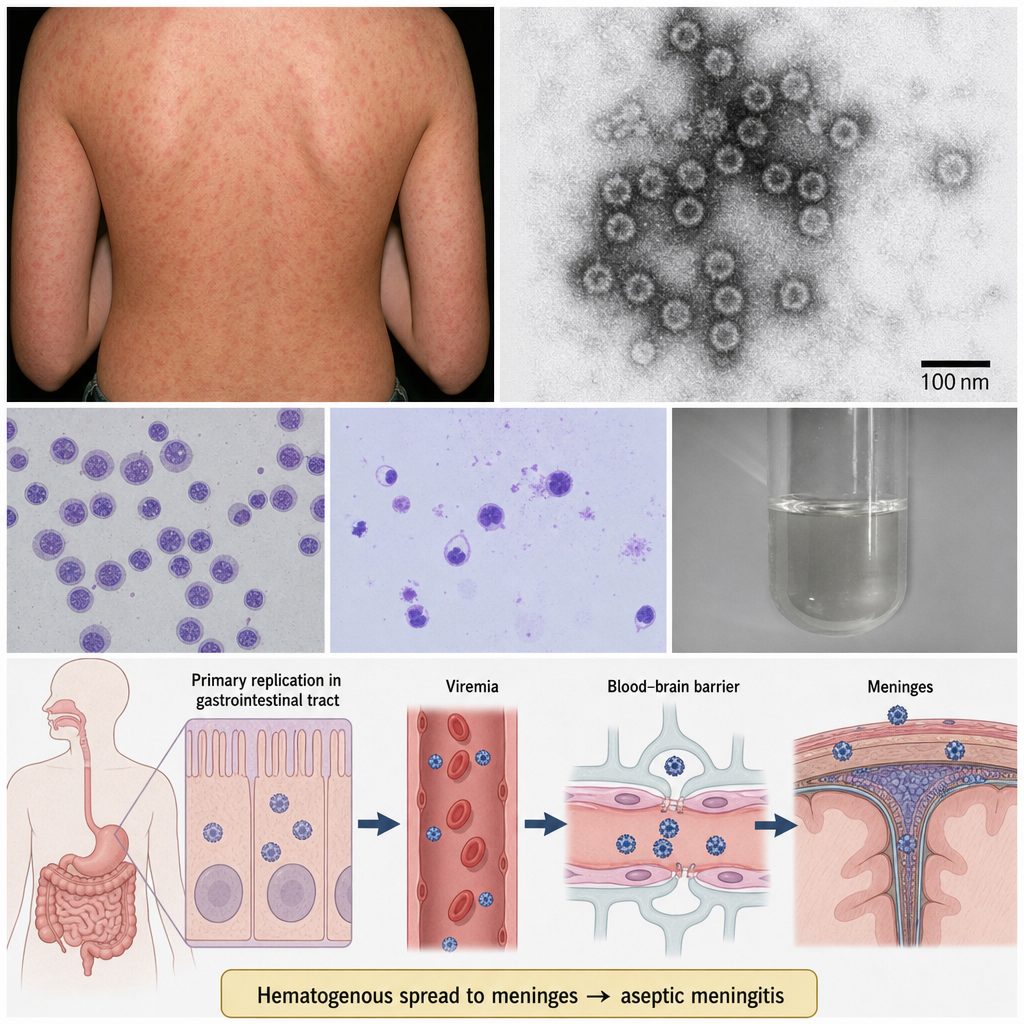
A viral particle is isolated from the cerebrospinal fluid of a 22-year-old immunocompetent college student presenting with aseptic meningitis, photophobia, and a maculopapular rash that began on the trunk and spread to the extremities. The particle is approximately 70 nm in diameter, icosahedral, non-enveloped, and contains a single-stranded positive-sense RNA genome. Which of the following best identifies this virus and its mechanism of central nervous system entry?
A 29-year-old pregnant woman with no prior antibiotic exposure presents with gonorrhea. Culture of Neisseria gonorrhoeae shows resistance to penicillin, tetracycline, and fluoroquinolones. Genetic testing reveals she has a strain with chromosomal mutations in penA (mosaic allele), mtrR promoter, and gyrA. She reports her partner recently returned from Southeast Asia. Apply epidemiologic and resistance mechanism knowledge to determine the most appropriate management and public health action.
A 67-year-old woman with persistent Enterococcus faecium bacteremia despite appropriate vancomycin therapy undergoes repeat culture. The isolate now shows vancomycin MIC of 128 μg/mL (previously 2 μg/mL). PCR testing reveals the presence of vanA gene cluster. Hospital epidemiology traces potential sources. What is the most likely mechanism by which this organism acquired high-level vancomycin resistance?
A 31-year-old man with acute myeloid leukemia develops neutropenic fever during chemotherapy. Blood cultures grow Pseudomonas aeruginosa resistant to all tested antibiotics including polymyxins (colistin). Genetic analysis shows mutations in pmrA and pmrB genes, as well as arnB gene. What mechanism best explains this organism's resistance to polymyxins, and what therapeutic implication does this have?
A 42-year-old woman with treatment-refractory pulmonary tuberculosis has documented resistance to rifampin, isoniazid, fluoroquinolones, and aminoglycosides. Whole genome sequencing reveals mutations in rpoB, katG, gyrA, rrs genes, and also shows a mutation in Rv0678 gene. Her treatment regimen includes bedaquiline. What is the clinical significance of the Rv0678 mutation in the context of her current therapy?
Practice by Chapter
Bacterial genome structure
Practice Questions
Horizontal gene transfer mechanisms
Practice Questions
Plasmids and mobile genetic elements
Practice Questions
Transposons and integrons
Practice Questions
Beta-lactamase types and mechanisms
Practice Questions
MRSA resistance mechanisms
Practice Questions
VRE resistance mechanisms
Practice Questions
Fluoroquinolone resistance
Practice Questions
Aminoglycoside resistance
Practice Questions
Multi-drug resistant gram-negatives
Practice Questions
Biofilm-associated resistance
Practice Questions
Evolution of antimicrobial resistance
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app