
Hospital-acquired infections — MCQs

On this page
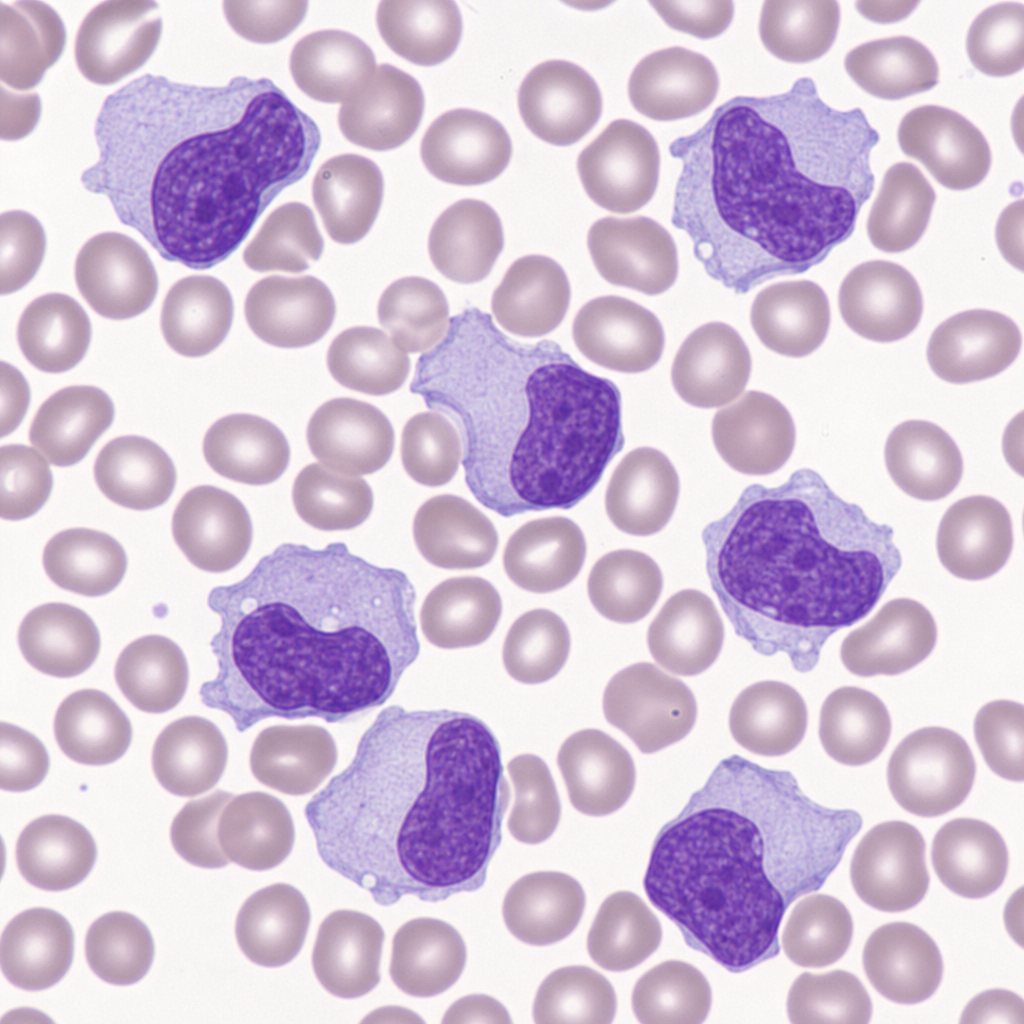
A 19-year-old college student presents with a 5-day history of fever, sore throat, and cervical lymphadenopathy. A heterophile antibody test is positive. A peripheral blood smear reveals large lymphocytes with abundant pale cytoplasm and irregular, folded nuclei that appear to indent around adjacent red blood cells. Which of the following surface markers would be found on the cells predominantly expanded in this patient's peripheral blood?
A surgical ICU has implemented multiple interventions over 18 months: chlorhexidine bathing, antibiotic stewardship, contact precautions for MRSA, and environmental cleaning protocols. Despite these efforts, MRSA surgical site infection rates remain unchanged at 8 per 1000 surgical procedures. Universal MRSA screening shows 15% of admitted patients are colonized. Evaluate the most effective evidence-based strategy to reduce MRSA SSI rates further.
A 70-year-old man with prosthetic aortic valve develops fever and bacteremia 3 weeks after valve replacement. Blood cultures grow Enterococcus faecium resistant to ampicillin and vancomycin (VRE). Susceptibilities show sensitivity to linezolid and daptomycin. TEE shows a small vegetation on the prosthetic valve. Creatinine is 1.8 mg/dL (baseline 1.0). Evaluate the optimal treatment strategy considering the infection location and drug characteristics.
A hospital implements a bundle to reduce catheter-associated urinary tract infections (CAUTI): daily review of catheter necessity, aseptic insertion technique, and proper maintenance. After 6 months, CAUTI rates decrease by 40% but then plateau. Compliance audits show 95% adherence to the bundle. The infection control team must evaluate the next intervention to achieve further reduction.
A 58-year-old woman with cirrhosis undergoes liver transplantation. On postoperative day 14, she develops fever, confusion, and abdominal pain. CT shows fluid collection near the biliary anastomosis. Aspiration yields purulent material. Culture grows Candida glabrata. She is on prophylactic fluconazole. Analyze the management failure and appropriate intervention.
An ICU experiences a cluster of 5 ventilator-associated pneumonia cases over 2 weeks. All isolates are Pseudomonas aeruginosa with identical antibiotic resistance patterns (resistant to cefepime, piperacillin-tazobactam, but susceptible to colistin). The affected patients are in different rooms. Environmental cultures from ventilator circuits are negative. Analyze the most likely source and transmission mechanism.
A 62-year-old man in the ICU for septic shock has been on broad-spectrum antibiotics (vancomycin, meropenem, micafungin) for 10 days. Initial blood cultures grew MRSA, now cleared. He develops new fever (38.8°C) and hypotension. Repeat blood cultures at 48 hours show no growth. He has a central line, Foley catheter, and endotracheal tube. Analysis of the clinical situation suggests which most likely explanation for persistent fever?
A 45-year-old diabetic woman develops fever and altered mental status 4 days after kidney transplantation. She is on tacrolimus and prednisone. Temperature is 39.4°C, BP 90/60 mmHg. Urinalysis shows WBCs and bacteria. Blood and urine cultures grow Escherichia coli resistant to ceftriaxone but susceptible to carbapenems, aminoglycosides, and trimethoprim-sulfamethoxazole. She has normal renal function. Apply the optimal long-term antibiotic choice.
A 72-year-old man undergoes colon resection for adenocarcinoma. On postoperative day 5, he develops watery diarrhea (8 episodes/day), abdominal cramping, and fever (38.5°C). He has been receiving cefoxitin prophylaxis extended postoperatively. WBC count is 18,000/μL. Stool studies are pending. Apply the most appropriate initial management.
A 55-year-old man with acute myeloid leukemia is hospitalized for chemotherapy. On day 7 of neutropenia (ANC 200/μL), he develops fever to 39.2°C and hypotension. Blood cultures from his central venous catheter grow gram-positive cocci in clusters. He has a history of anaphylaxis to penicillin with angioedema. Apply the most appropriate antibiotic therapy.
Practice by Chapter
Catheter-associated urinary tract infections
Practice Questions
Central line-associated bloodstream infections
Practice Questions
Ventilator-associated pneumonia
Practice Questions
Surgical site infections
Practice Questions
Clostridium difficile infection
Practice Questions
Multi-drug resistant organism transmission
Practice Questions
Environmental reservoirs in healthcare settings
Practice Questions
Infection control practices
Practice Questions
Outbreak investigation
Practice Questions
Surveillance methodologies
Practice Questions
Hand hygiene compliance
Practice Questions
Isolation precautions
Practice Questions
Prevention bundles and checklists
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app