
HIV — MCQs

On this page
A 49-year-old homeless man comes to the emergency department because of fatigue, cough, and worsening shortness of breath for 2 weeks. He was diagnosed with HIV-infection 25 years ago but has never had any symptoms. He has always refused to take antiretroviral medication. Pulmonary examination shows diffuse crackles over bilateral lower lung fields. An x-ray of the chest shows diffuse, symmetrical interstitial infiltrates. His serum level of beta-d-glucan is elevated. Further testing shows a heterozygous mutation that prevents entry of HIV into macrophages. Which of the following proteins is most likely affected by the mutation in this patient?
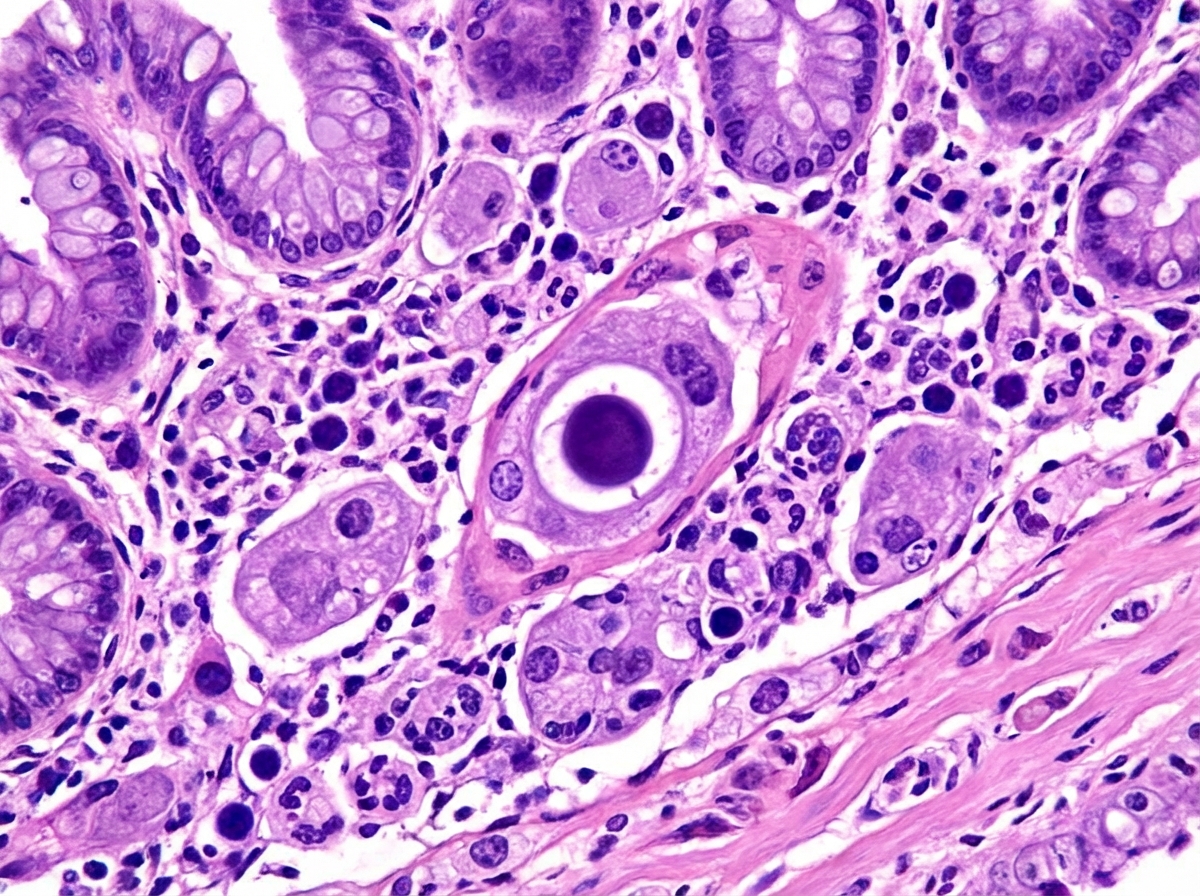
A 45-year-old man comes to the physician because of a 3-week history of progressive diarrhea and a 2.2-kg (5-lb) weight loss. During the past week, he has had six small bloody stools daily. He is employed as a sales manager and regularly flies to South America. He has HIV, gastroesophageal reflux disease, and hypertension. Current medications include chlorthalidone, omeprazole, emtricitabine, tenofovir, and efavirenz. He reports taking efavirenz irregularly. He is 175 cm (5 ft 9 in) tall and weighs 64 kg (143 lb); BMI is 22 kg/m2. His temperature is 38.1°C (100.6°F), pulse is 91/min, and blood pressure is 116/69 mm Hg. The abdomen is scaphoid. Bowel sounds are normal. His CD4+ T-lymphocyte count is 44/mm3 (N ≥ 500), leukocyte count is 6,000/mm3, and erythrocyte sedimentation rate is 12 mm/h. Colonoscopy shows areas of inflammation scattered throughout the colon with friability, granularity, and shallow linear ulcerations. The intervening mucosa between areas of inflammation appears normal. A biopsy specimen is shown. Which of the following is the most likely cause of this patient's symptoms?
A 45-year-old man with a history of poorly controlled human immunodeficiency virus (HIV) infection presents to the emergency room complaining of clumsiness and weakness. He reports a 3-month history of worsening balance, asymmetric muscle weakness, and speech difficulties. He recently returned from a trip to Guatemala to visit his family. He has been poorly compliant with his anti-retroviral therapy and his most recent CD4 count was 195. His history is also notable for rheumatoid arthritis and hepatitis C. His temperature is 99°F (37.2°C), blood pressure is 140/90 mmHg, pulse is 95/min, and respirations are 18/min. On exam, he has 4/5 strength in his right upper extremity, 5/5 strength in his left upper extremity, 5/5 strength in his right lower extremity, and 3/5 strength in his left lower extremity. His speech is disjointed with intermittent long pauses between words. Vision is 20/100 in the left eye and 20/40 in his right eye; previously, his eyesight was 20/30 bilaterally. This patient most likely has a condition caused by which of the following types of pathogens?
A 45-year-old man comes to the physician for the evaluation of painful swallowing and retrosternal pain over the past 2 days. He was recently diagnosed with HIV infection, for which he now takes tenofovir, emtricitabine, and raltegravir. There is no family history of serious illness. He has smoked one pack of cigarettes daily for the past 20 years. He drinks 2–3 beers per day. He does not use illicit drugs. Vital signs are within normal limits. Physical examination of the oral cavity shows no abnormalities. The patient's CD4+ T-lymphocyte count is 80/mm3 (normal ≥ 500). Empiric treatment is started. Two weeks later, he reports no improvement in his symptoms. Esophagogastroduodenoscopy is performed and shows multiple well-circumscribed, round, superficial ulcers in the upper esophagus. Which of the following is the most likely underlying cause of this patient's symptoms?
A laboratory method uses chromogenic substrates, in which a reaction may be interpreted according to an enzyme-mediated color change. The detection of which of the substances below is routinely used in clinical practice and applies the above-described method?
A 20-year-old female arrives at the urgent care clinic at her university’s health plan asking for an HIV test. She is an undergraduate at the university and just started having sexual intercourse with her new boyfriend. They use protection only occasionally so she wants to get tested to make sure everything is okay. She has never been tested for STDs before. She reports no symptoms and has not seen a physician regularly for any medical conditions in the past. Her family history is uncertain because she was adopted. Her HIV immunoassay and HIV-1/HIV-2 differentiation immunoassay both come back positive. She asks on the phone, “Doctor, tell it to me straight. Do I have AIDS?” Which of the following is the most accurate response?
A 48-year-old woman is brought to her primary care physician by her sister who is concerned about a deterioration in the patient's general status. The patient was diagnosed with HIV 7 years ago. She says that her last T cell count was "good enough", so she has been skipping every other dose of her antiretroviral medications and trimethoprim-sulfamethoxazole. Her sister has had to drive her home from work several times this month because she has become disoriented and confused about her surroundings. Motor strength is 4/5 on the right and 3/5 on the left. She is able to walk unassisted, but her gait appears mildly uncoordinated. There is diplopia when the right eye is covered. Her CD4 count is 75 cells/µL. MRI shows numerous asymmetric, hyperintense, non-enhancing lesions bilaterally without mass effect. Brain biopsy shows demyelination and atypical astrocytes. Which of the following is most likely responsible for this patient's current condition?
A 37-year-old man comes to the physician because of fever, night sweats, malaise, dyspnea, and a productive cough with bloody sputum for 4 days. He was diagnosed with HIV infection 15 years ago and has not been compliant with his medication regimen. Physical examination shows diminished breath sounds over the left lung fields. An x-ray of the chest shows an ill-defined lesion in the upper lobe of the left lung. A CT-guided biopsy of the lesion is performed; a photomicrograph of the biopsy specimen stained with mucicarmine is shown. Which of the following is the most likely causal organism?
A 32-year-old man comes to the physician with difficulty swallowing for several weeks. Examination of the oropharynx shows lesions on palate and tongue that can be easily scraped off. An image of the lesions is shown. Which of the following is a risk factor for this patient's findings?

During an experiment conducted to alter the infectivity of common viruses that affect humans, an investigator successfully increases the host range of human immunodeficiency virus (HIV). The new strain of the virus can infect fibroblast-like cells in addition to the usual target of HIV. Which of the following is the most likely explanation for the increase in the host range of the virus?
Practice by Chapter
HIV structure and replication cycle
Practice Questions
HIV transmission and epidemiology
Practice Questions
Acute HIV infection
Practice Questions
CD4 monitoring and viral load
Practice Questions
Opportunistic infections in HIV/AIDS
Practice Questions
Antiretroviral therapy principles
Practice Questions
NRTI, NNRTI, PI, INSTI, and entry inhibitors
Practice Questions
HIV resistance testing
Practice Questions
HIV prevention strategies
Practice Questions
HIV-associated malignancies
Practice Questions
HIV in pregnancy and vertical transmission
Practice Questions
HIV co-infections (HBV, HCV, TB)
Practice Questions
HIV cure research
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app