
HIV-associated malignancies — MCQs

A 58-year-old woman with HIV infection is brought to the emergency department because of a 2-week history of headaches, blurred vision, and confusion. Her current medications include antiretroviral therapy and trimethoprim-sulfamethoxazole. Neurological examination shows ataxia and memory impairment. Her CD4+ T-lymphocyte count is 90/μL. Cerebrospinal fluid analysis shows lymphocytic predominant pleocytosis, and PCR is positive for Epstein-Barr virus DNA. An MRI of the brain with contrast shows a solitary, weakly ring-enhancing lesion with well-defined borders involving the corpus callosum. Which of the following is the most likely diagnosis?
A 52-year-old man is brought to the emergency department because of headaches, vertigo, and changes to his personality for the past few weeks. He was diagnosed with HIV 14 years ago and was started on antiretroviral therapy at that time. Medical records from one month ago indicate that he followed his medication schedule inconsistently. Since then, he has been regularly taking his antiretroviral medications and trimethoprim-sulfamethoxazole. His vital signs are within normal limits. Neurological examination shows ataxia and apathy. Mini-Mental State Examination score is 15/30. Laboratory studies show: Hemoglobin 12.5 g/dL Leukocyte count 8400/mm3 Segmented neutrophils 80% Eosinophils 1% Lymphocytes 17% Monocytes 2% CD4+ T-lymphocytes 90/μL Platelet count 328,000/mm3 An MRI of the brain with contrast shows a solitary ring-enhancing lesion involving the corpus callosum and measuring 4.5 cm in diameter. A lumbar puncture with subsequent cerebrospinal fluid analysis shows slight pleocytosis, and PCR is positive for Epstein-Barr virus DNA. Which of the following is the most likely diagnosis?
A 45-year-old man comes to the emergency department because of chills and numerous skin lesions for 1 week. He has also had watery diarrhea, nausea, and abdominal pain for the past 2 weeks. The skin lesions are nonpruritic and painless. He was diagnosed with HIV infection approximately 20 years ago. He has not taken any medications for over 5 years. He sleeps in homeless shelters and parks. Vital signs are within normal limits. Examination shows several bright red, friable nodules on his face, trunk, extremities. The liver is palpated 3 cm below the right costal margin. His CD4+ T-lymphocyte count is 180/mm3 (N ≥ 500). A rapid plasma reagin test is negative. Abdominal ultrasonography shows hepatomegaly and a single intrahepatic 1.0 x 1.2-cm hypodense lesion. Biopsy of a skin lesion shows vascular proliferation and abundant neutrophils. Which of the following is the most likely causal organism?
A 41-year-old man with HIV comes to the physician because of rectal bleeding and itching for 2 weeks. During this period, he has also had pain with defecation. Four months ago, he was diagnosed with anogenital warts that were treated with cryotherapy. Over the past year, he has been sexually active with 3 male partners. He uses condoms inconsistently. Current medications are zidovudine, emtricitabine, and efavirenz. Digital rectal examination and anoscopy show an exophytic mass on the anal margin that is protruding into the anal canal. The mass is tender to palpation and bleeds easily on contact. Laboratory studies show a leukocyte count of 7,600/mm3 and a CD4+ T-lymphocyte count of 410/mm3 (N ≥ 500). A biopsy specimen of the lesion shows a well-differentiated squamous cell carcinoma. Which of the following cellular processes was most likely involved in the pathogenesis of this patient's malignancy?
A 63-year-old man presents to his primary care physician because he has been having headaches and hearing loss. In addition, he says that he has been having difficulty opening his jaw to eat and recurrent middle ear infections. Physical exam reveals enlarged neck lymph nodes and a mass in the nasopharynx. Biopsy of the mass reveals undifferentiated squamous epithelial cells. The organism that is most likely associated with this patient's disease is also associated with which of the following disorders?
A 44-year-old man with HIV comes to the physician for a routine follow-up examination. He has been noncompliant with his antiretroviral medication regimen for several years. He appears chronically ill and fatigued. CD4+ T-lymphocyte count is 180/mm³ (N ≥ 500). Further evaluation of this patient is most likely to show which of the following findings?
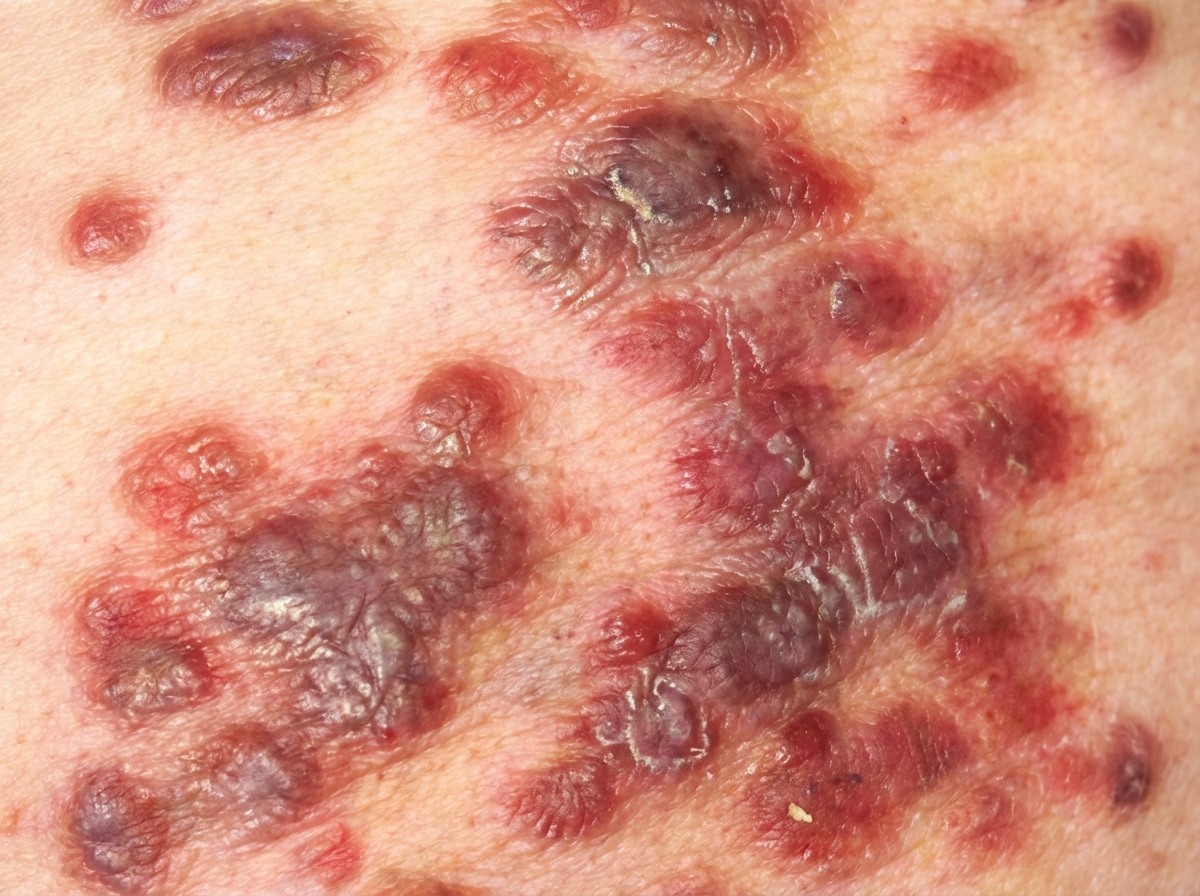
A 52-year-old woman presents to a local hospital complaining about a rash on her face and torso, as well as night sweats, low-grade fever, diarrhea, and unintentional weight loss. Her personal history is relevant for homelessness; she also has a history of risky behaviors such as the use and abuse of intravenous drugs, and unprotected intercourse with multiple sexual partners. Upon physical examination, well-demarcated violaceous plaques and papules distributed on her face and back are visible (see image below). Additional findings include fine reticular and interstitial changes on a chest radiograph, a CD4+ count of 50 cells/mm3, and positive HIV serology. Which of the following is the most likely etiology of this patient's dermatological condition?
A 24-year-old male presents to the emergency room with a cough and shortness of breath for the past 3 weeks. You diagnose Pneumocystis jiroveci pneumonia (PCP). An assay of the patient's serum reveals the presence of viral protein p24. Which of the following viral genes codes for this protein?
A 44-year-old with a past medical history significant for human immunodeficiency virus infection presents to the emergency department after he was found to be experiencing worsening confusion. The patient was noted to be disoriented by residents and staff at the homeless shelter where he resides. On presentation he reports headache and muscle aches but is unable to provide more information. His temperature is 102.2°F (39°C), blood pressure is 112/71 mmHg, pulse is 115/min, and respirations are 24/min. Knee extension with hips flexed produces significant resistance and pain. A lumbar puncture is performed with the following results: Opening pressure: Normal Fluid color: Clear Cell count: Increased lymphocytes Protein: Slightly elevated Which of the following is the most likely cause of this patient's symptoms?
A 49-year-old homeless man comes to the emergency department because of fatigue, cough, and worsening shortness of breath for 2 weeks. He was diagnosed with HIV-infection 25 years ago but has never had any symptoms. He has always refused to take antiretroviral medication. Pulmonary examination shows diffuse crackles over bilateral lower lung fields. An x-ray of the chest shows diffuse, symmetrical interstitial infiltrates. His serum level of beta-d-glucan is elevated. Further testing shows a heterozygous mutation that prevents entry of HIV into macrophages. Which of the following proteins is most likely affected by the mutation in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app