
Hepatitis B/C — MCQs

On this page
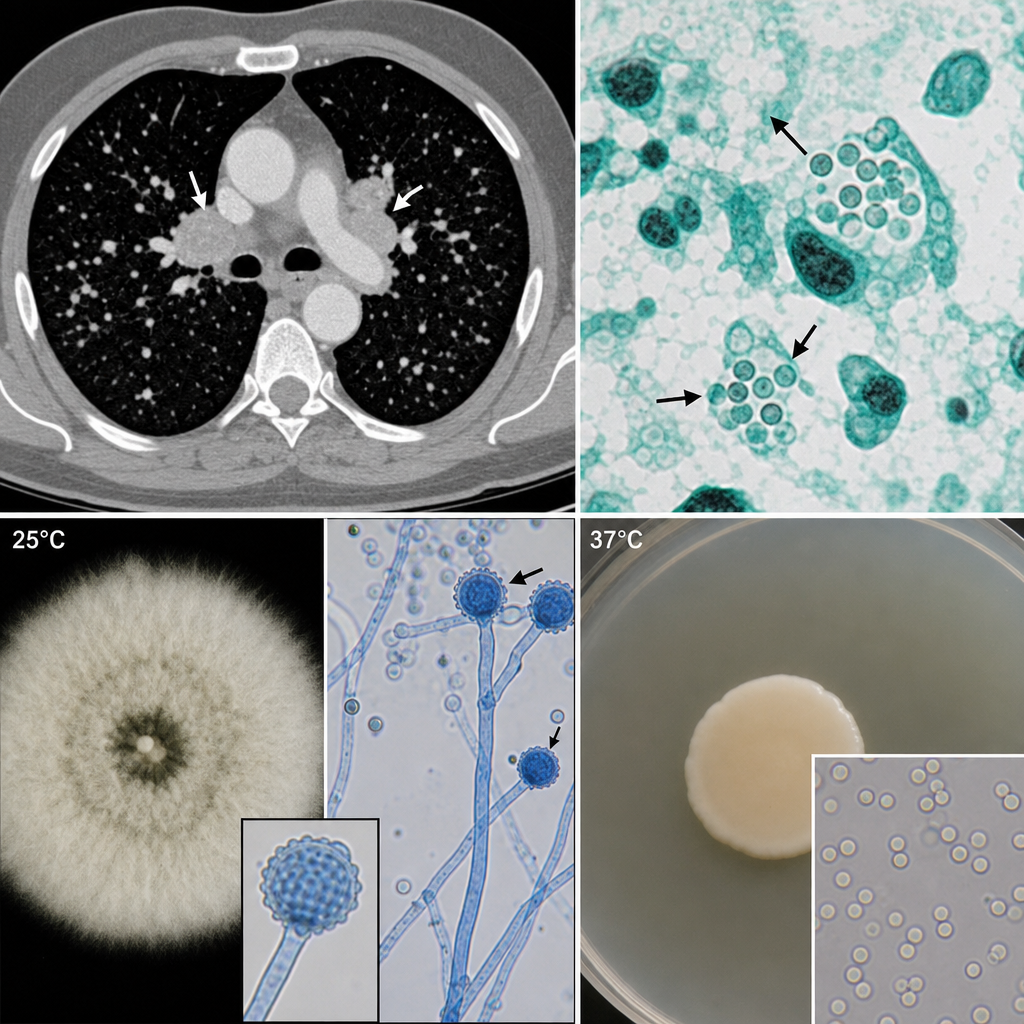
A 45-year-old immunocompetent woman from rural Ohio presents with a 3-week history of low-grade fever, night sweats, and a non-productive cough. She recently helped clean out an old barn near a dried river bed. Chest CT reveals mediastinal lymphadenopathy and multiple small pulmonary nodules. A bronchoalveolar lavage specimen is sent for fungal culture. At 25°C, the organism grows as a mold with tuberculate macroconidia. At 37°C, the same isolate grows as small yeast cells (2–4 µm) found inside macrophages on cytology. A colleague suggests the presentation is more consistent with Blastomyces dermatitidis based on the geographic exposure. Which of the following findings would most definitively argue against the colleague's proposed organism and confirm the correct diagnosis?
A group of researchers conducted various studies on hepatitis C incidence and prevalence. They noticed that there is a high prevalence of hepatitis C in third-world countries, where it has a significant impact on the quality of life of the infected individual. The research group made several attempts to produce a vaccine that prevents hepatitis C infection but all attempts failed. Which of the following would most likely be the reason for the failure to produce a vaccine?
A 13-year-old boy presents to the pediatrician with yellow discoloration of the sclerae since yesterday, and dark-colored urine for 2 days. A detailed history is taken and reveals that he had a cough, cold, and fever the week before the onset of the current symptoms, and was treated with over-the-counter medications. He reports an improvement in his upper respiratory symptoms but has been experiencing fatigue, nausea, and poor appetite since then. There is no past history of recurrent nausea, vomiting, jaundice or abdominal pain, and he has not received any blood transfusion. In addition, he frequently eats at a roadside restaurant near his school. His growth and development are normal for his age and sex. The temperature is 37.9°C (100.2°F), pulse is 96/min, blood pressure is 110/70 mm Hg, and the respiratory rate is 22/min. The physical examination shows icterus. The examination of the abdomen reveals tender hepatomegaly with the liver having a firm, sharp, and smooth edge. The laboratory test results are as follows: Hemoglobin 14.2 g/dL WBC (white blood cell) 10,500/mm3 Differential leukocyte count Segmented neutrophils 56% Bands 4% Lymphocytes 35% Eosinophils 2% Basophils 0% Monocytes 3% Platelet count 270,000/mm3 Serum total bilirubin 8.4 mg/dL Serum direct bilirubin 7.8 mg/dL Serum alanine aminotransferase 350 U/L Serum alkaline phosphatase 95 U/L Prothrombin time 20 seconds Which of the following laboratory tests is most likely used to diagnose the condition of this patient?
A scientist is studying the replication sequences of a number of different viruses. He observes that one particular virus he is studying creates a single stranded DNA from an RNA template during its replication sequence. Which of the following viruses is he most likely observing?
A previously healthy 25-year-old woman comes to the physician because of a one-week history of diffuse abdominal pain. Her temperature is 39.1°C (102.3°F). Physical examination shows numerous scars and excoriations along both arms, scleral icterus, and tender hepatomegaly. Serum studies show: Alanine aminotransferase 927 U/L Aspartate aminotransferase 796 U/L Hepatitis B surface antigen positive Hepatitis B surface antibody negative Anti-hepatitis B core antibody positive Hepatitis C antibody negative Which of the following is the most likely outcome of this patient's infection?
A 25-year-old construction worker presents to the office due to a yellowish discoloration of his skin and eyes for the past 2 weeks. He also complains of nausea and loss of appetite for the same duration. The past medical history is insignificant. He is a smoker, but recently has grown a distaste for smoking. The vital signs include: heart rate 83/min, respiratory rate 13/min, temperature 36.5°C (97.7°F), and blood pressure 111/74 mm Hg. On physical examination, there is mild hepatomegaly. The results of the hepatitis viral panel are as follows: Anti-HAV IgM positive HBsAg negative IgM anti-HBc negative Anti-HCV negative HCV-RNA negative Anti-HDV negative Anti-HEV negative What is the most common mode of transmission for this patient’s diagnosis?
A 32-year-old man presents to the physician with a history of fever, malaise, and arthralgia in the large joints for the last 2 months. He also mentions that his appetite has been significantly decreased during this period, and he has lost considerable weight. He also informs the physician that he often experiences tingling and numbness in his right upper limb, and his urine is also dark in color. The past medical records show that he was diagnosed with an infection 7 months before and recovered well. On physical examination, the temperature is 37.7°C (99.8°F), the pulse rate is 86/min, the respiratory rate is 14/min, and the blood pressure is 130/94 mm Hg. Which of the following infections has most likely caused the condition the patient is suffering from?
A 28-year-old man comes to the physician because of progressively worsening fatigue, nausea, and right upper quadrant pain. He has a history of intravenous heroin use. Serum Anti-HBc is positive. Further analysis of the Anti-HBc immunoglobulin in this acute presentation is most likely to show which of the following properties?
A 27-year-old woman who recently emigrated from Brazil comes to the physician because of fever, fatigue, decreased appetite, and mild abdominal discomfort. She has not seen a physician in several years and her immunization status is unknown. She drinks 2 alcoholic beverages on the weekends and does not use illicit drugs. She is sexually active with several male partners and uses condoms inconsistently. Her temperature is 38°C (99.8°F). Physical examination shows right upper quadrant tenderness and scleral icterus. Serology confirms acute infection with a virus that has partially double-stranded, circular DNA. Which of the following is most likely involved in the replication cycle of this virus?
A 57-year-old man comes to the physician because of generalized malaise, yellowish discoloration of the eyes, and pruritus on the back of his hands that worsens when exposed to sunlight for the past several months. He has not seen a physician in 15 years. Physical examination shows scleral icterus and mild jaundice. There is a purpuric rash with several small vesicles and hyperpigmented lesions on the dorsum of both hands. The causal pathogen of this patient's underlying condition was most likely acquired in which of the following ways?
Practice by Chapter
HBV structure and replication
Practice Questions
HBV serological markers
Practice Questions
Acute hepatitis B
Practice Questions
Chronic hepatitis B phases
Practice Questions
HBV treatment indications and options
Practice Questions
HBV vaccination and prevention
Practice Questions
HCV structure and genotypes
Practice Questions
HCV diagnostic testing
Practice Questions
Natural history of HCV infection
Practice Questions
Direct-acting antivirals for HCV
Practice Questions
HCV resistance and treatment failure
Practice Questions
HBV/HCV co-infection
Practice Questions
HCC screening in viral hepatitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app