
Gram-positive — MCQs

On this page
A 45-year-old woman presents with fever, pain, and swelling of the right leg. She says that her right leg swelling has gradually worsened over the last 2 weeks. She has also noted worsening fatigue and anorexia. Two days ago, she developed a low-grade fever. Her past medical history is significant for type 2 diabetes mellitus diagnosed 5 years ago and managed with metformin. Her temperature is 38.0°C (100.4°F), pulse is 110/min, blood pressure is 110/72 mm Hg, and respiratory rate is 16/min. On physical examination, there is a painful swelling of the right lower extremity extending to just below the knee joint. The overlying skin is tense, glossy, erythematous, and warm to touch. A diagnosis of cellulitis is established and appropriate antibiotics are started. Which of the following best describes the organism most likely responsible for this patient’s condition?
A 24-year-old male is brought into the emergency department complaining of chills, headaches, and malaise for several days. He also states that he experiences shortness of breath when climbing two flights of stairs in his home. He admits to occasionally using intravenous drugs during the previous year. On exam, his vital signs are temperature 39.2° C, heart rate 108/min, blood pressure 124/82 mm Hg, respiratory rate 20/min, and oxygen saturation 98% on room air. A holosystolic murmur is heard near the lower left sternal border. An echocardiogram confirms vegetations on the tricuspid valve. What is the most likely causative organism of this patient's condition?
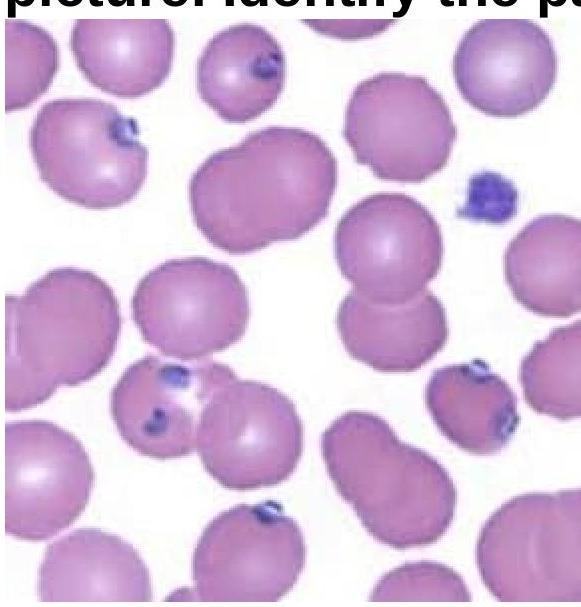
A 30-year-old man is brought to the emergency department with complaints of fevers to 39.0℃ (102.2℉) and diarrhea for the past 12 hours. There is no history of headaches, vomiting, or loss of consciousness. The past medical history is unobtainable because the patient recently immigrated from abroad and has a language barrier, but his wife says that her husband had a motor vehicle accident when he was a teenager that required emergent surgery. He is transferred to the ICU after a few hours in the ED due to dyspnea, cyanosis, and hemodynamic collapse. There are no signs of a meningeal infection. The blood pressure is 70/30 mm Hg at the time of transfer. A chest X-ray at the time of admission shows interstitial infiltrates without homogeneous opacities. The initial laboratory results reveal metabolic acidosis, leukopenia with a count of 2000/mm3, thrombocytopenia (15,000/mm3), and a coagulation profile suggesting disseminated intravascular coagulation. A peripheral smear is performed as shown in the accompanying image. Despite ventilatory support, administration of intravenous fluids, antibiotics, and vasopressor agents, the patient dies the next day. Which of the following organisms is the most likely cause for the patient's condition?
A 55-year-old IV drug user comes into the emergency department after four days of pain in his right ankle. The patient is lethargic and unable to answer any questions about his medical history. His vitals are HR 110, T 101.5, RR 20, BP 100/60. His physical exam is notable for track marks in his toes and his right ankle is erythematous and swollen. Moving any part of the right foot creates a 10/10 pain. A radiograph reveals no evidence of fractures. A Gram stain of the joint fluid aspirate demonstrates purple cocci in clusters. The fluid is yellow, opaque, with more than 70,000 cells/mm^3 (80% neutrophils). What is the most likely diagnosis?
A 52-year-old man is brought to the emergency department after being found down on the sidewalk. On presentation, he is found to have overdosed on opioids so he is given naloxone and quickly recovers. Physical exam also reveals lumps on his neck and face that are covered by small yellow granules. These lumps are slowly draining yellow pus-like fluid. He says that these lumps have been present for several months, but he has ignored them because he has not had any fever or pain from the lumps. He does not recall the last time he visited a primary care physician or a dentist. Oral exam reveals multiple cavities and abscesses. The most likely cause of this patient's facial lumps has which of the following characteristics?
A team of intensivists working in a private intensive care unit (ICU) observe that the clinical efficacy of vancomycin is low, and proven nosocomial infections have increased progressively over the past year. A clinical microbiologist is invited to conduct a bacteriological audit of the ICU. He analyzes the microbiological reports of all patients treated with vancomycin over the last 2 years and takes relevant samples from the ICU for culture and antibiotic sensitivity analysis. The audit concludes that there is an increased incidence of vancomycin-resistant Enterococcus fecalis infections. Which of the following mechanisms best explains the changes that took place in the bacteria?
A 69-year-old woman is brought to the emergency department by her husband because of a 1-day history of fever, shortness of breath, dizziness, and cough productive of purulent sputum. Six days ago, she developed malaise, headache, sore throat, and myalgias that improved initially. Her temperature is 39.3°C (102.7°F) and blood pressure is 84/56 mm Hg. Examination shows an erythematous, desquamating rash of the distal extremities. A sputum culture grows gram-positive, coagulase-positive cocci in clusters. The most likely causal organism of this patient's current symptoms produces a virulence factor with which of the following functions?
A 35-year-old man comes to the emergency room for severe left leg pain several hours after injuring himself on a gardening tool. His temperature is 39°C (102.2°F) and his pulse is 105/min. Physical examination of the left leg shows a small laceration on the ankle surrounded by dusky skin and overlying bullae extending to the posterior thigh. There is a crackling sound when the skin is palpated. Surgical exploration shows necrosis of the gastrocnemius muscles and surrounding tissues. Tissue culture shows anaerobic gram-positive rods and a double zone of hemolysis on blood agar. Which of the following best describes the mechanism of cellular damage caused by the responsible pathogen?
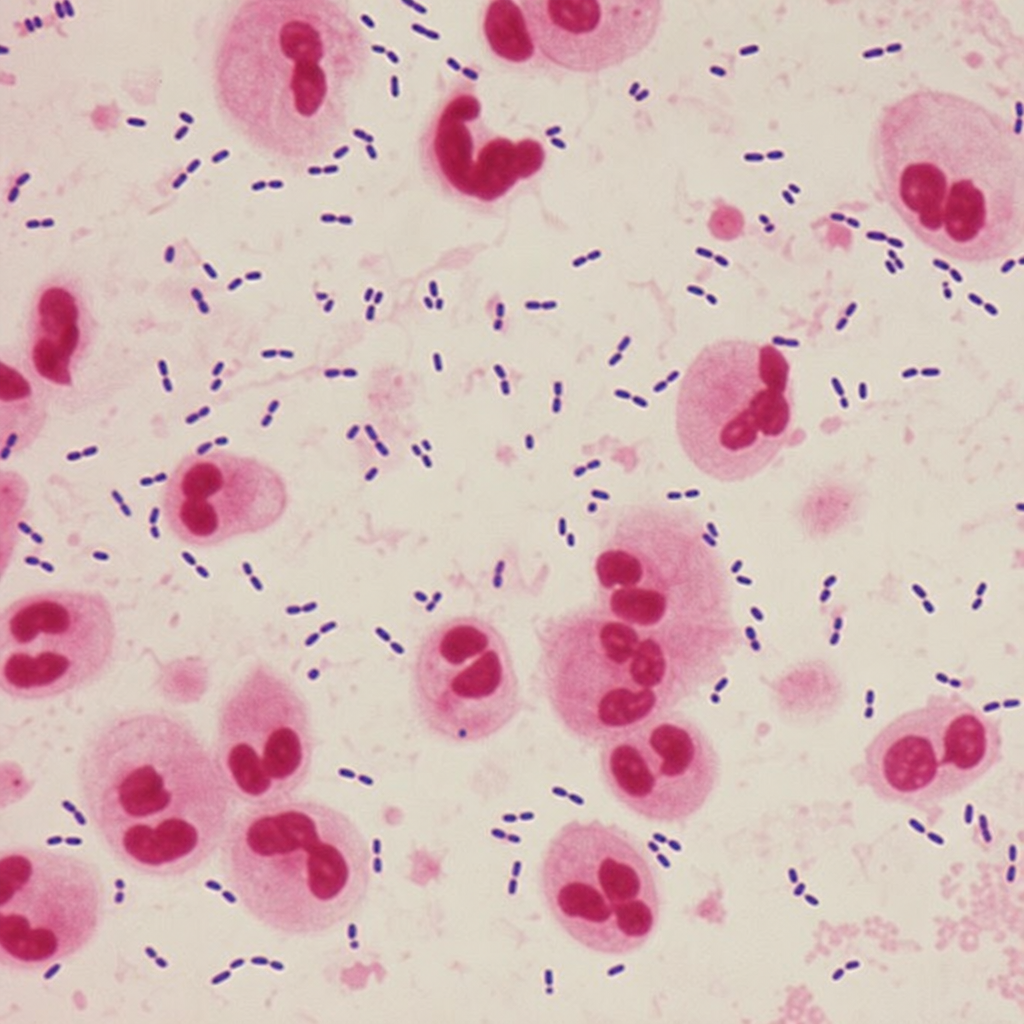
A 60-year-old man presents with fever and cough productive of rust-colored sputum and is diagnosed with community acquired pneumonia. The causative organism is isolated, and a Gram stain is shown in Figure 1. Which of the following most correctly describes additional features of the most likely causative organism?
An 18-month-old boy presents to the emergency department for malaise. The boy’s parents report worsening fatigue for 3 days with associated irritability and anorexia. The patient’s newborn screening revealed a point mutation in the beta-globin gene but the patient has otherwise been healthy since birth. On physical exam, his temperature is 102.4°F (39.1°C), blood pressure is 78/42 mmHg, pulse is 124/min, and respirations are 32/min. The child is tired-appearing and difficult to soothe. Laboratory testing is performed and reveals the following: Serum: Na+: 137 mEq/L Cl-: 100 mEq/L K+: 4.4 mEq/L HCO3-: 24 mEq/L Urea nitrogen: 16 mg/dL Creatinine: 0.9 mg/dL Glucose: 96 mg/dL Leukocyte count: 19,300/mm^3 with normal differential Hemoglobin: 7.8 g/dL Hematocrit: 21% Mean corpuscular volume: 82 um^3 Platelet count: 324,000/mm^3 Reticulocyte index: 3.6% Which of the following is the most likely causative organism for this patient's presentation?
Practice by Chapter
Staphylococcus aureus
Practice Questions
Coagulase-negative staphylococci
Practice Questions
Streptococcus pneumoniae
Practice Questions
Group A streptococci
Practice Questions
Group B streptococci
Practice Questions
Viridans group streptococci
Practice Questions
Enterococci
Practice Questions
Bacillus species
Practice Questions
Listeria monocytogenes
Practice Questions
Corynebacterium species
Practice Questions
Clostridium species
Practice Questions
Actinomyces and Nocardia
Practice Questions
MRSA and VRE
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app