
Group B streptococci — MCQs

A neonate born at 33 weeks is transferred to the NICU after a complicated pregnancy and C-section. A week after being admitted, he developed a fever and became lethargic and minimally responsive to stimuli. A lumbar puncture is performed that reveals the following: Appearance Cloudy Protein 64 mg/dL Glucose 22 mg/dL Pressure 330 mm H20 Cells 295 cells/mm³ (> 90% PMN) A specimen is sent to microbiology and reveals gram-negative rods. Which of the following is the next appropriate step in management?
A 14-year-old male is brought to the Emergency Department by his mother. She is worried because his face has become puffy and his urine has turned a tea-color. Patient history reveals the child recently suffered from a sore throat. The physician suspects a bacterial infection. Which of the following describes the likely bacteria responsible?
A 27-year-old woman, gravida 2, para 1, at 37 weeks' gestation is admitted to the hospital in active labor. She has received routine prenatal care, but she has not been tested for group B streptococcal (GBS) colonization. Pregnancy and delivery of her first child were complicated by an infection with GBS that resulted in sepsis in the newborn. Current medications include folic acid and a multivitamin. Vital signs are within normal limits. The abdomen is nontender and contractions are felt every 4 minutes. There is clear amniotic fluid pooling in the vagina. The fetus is in a cephalic presentation. The fetal heart rate is 140/min. Which of the following is the most appropriate next step in management?
A 27-year-old woman, gravida 2, para 1, at 36 weeks' gestation comes to the physician for a prenatal visit. She feels well. Fetal movements are adequate. This is her 7th prenatal visit. She had an ultrasound scan performed 1 month ago that showed a live intrauterine pregnancy consistent with a 32-week gestation with no anomalies. She had a Pap smear performed 1 year ago, which was normal. Vital signs are within normal limits. Pelvic examination shows a uterus consistent in size with a 36-week gestation. Her blood group and type is A negative. Which of the following is the most appropriate next step in management?
You are treating a neonate with meningitis using ampicillin and a second antibiotic, X, that is known to cause ototoxicity. What is the mechanism of antibiotic X?
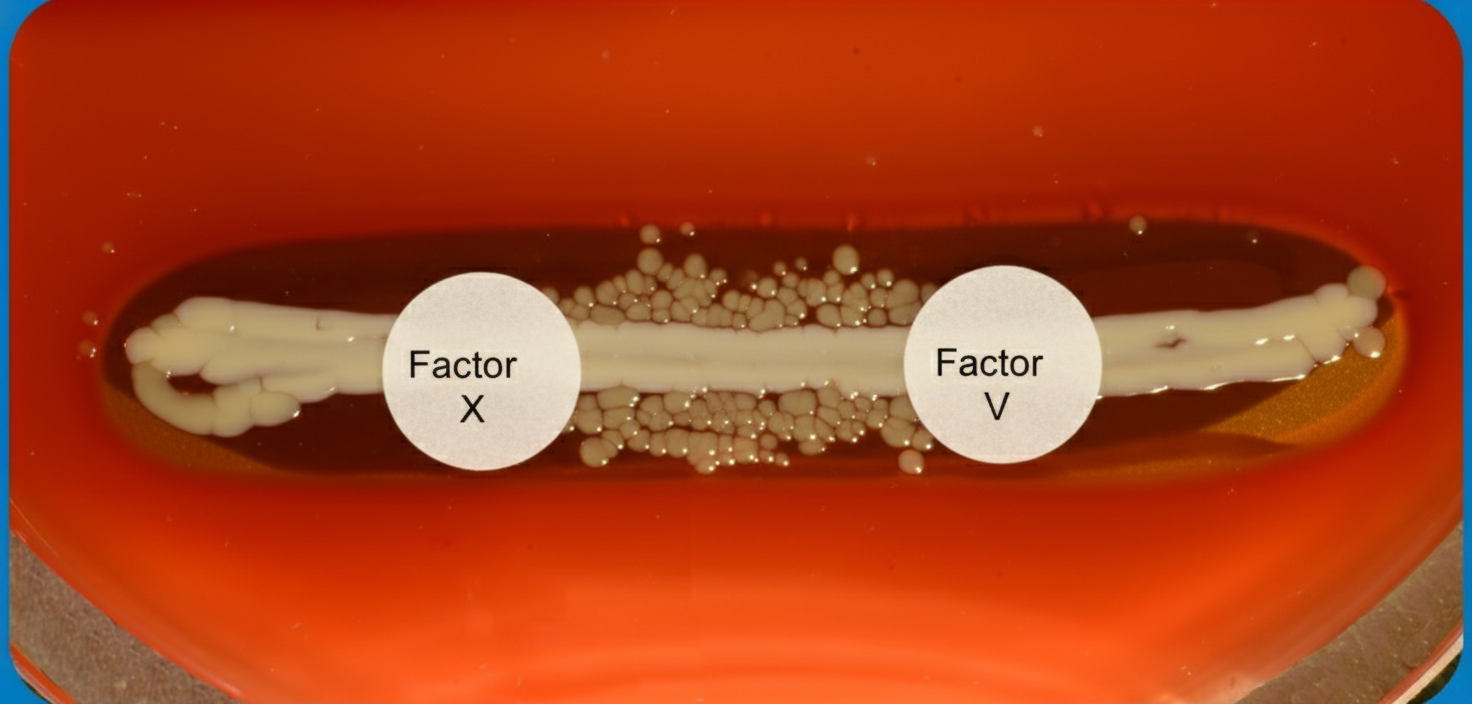
A 6-month old child is brought to the ER by parents for one day of fever, decreased feeding, and lethargy. They report that neither she nor her siblings are immunized due to their concerns about vaccinations. On exam, the infant is toxic-appearing. Antibiotics are started and lumbar puncture reveals bacterial meningitis caused by a gram-negative, encapsulated organism that requires chocolate agar and the two factors shown in Image A for growth. Which organism does this best describe?
A 62-year-old woman presents to the emergency department for evaluation of a spreading skin infection that began from an ulcer on her foot. The patient has type 2 diabetes mellitus that is poorly controlled. On examination, there is redness and erythema to the lower limb with skin breakdown along an extensive portion of the leg. The patient’s tissues separate readily from the fascial plane, prompting a diagnosis of necrotizing fasciitis. What is the exotoxin most likely associated with this patient’s presentation?
A person presents to the hospital with fever and chills. Fever profile is ordered and is found to be negative for malaria and dengue. Rk39 test is found to be positive. What is the treatment of choice?
A 32-year-old man comes to the physician with difficulty swallowing for several weeks. Examination of the oropharynx shows lesions on palate and tongue that can be easily scraped off. An image of the lesions is shown. Which of the following is a risk factor for this patient's findings?

A 24-hour-old newborn presents to the emergency department after a home birth because of fever, irritability alternating with lethargy, and poor feeding. The patient’s mother says symptoms acutely onset 12 hours ago and have not improved. No significant past medical history. His mother did not receive any prenatal care, and she had rupture of membranes 20 hours prior to delivery. His vital signs include: heart rate 150/min, respiratory rate 65/min, temperature 39.0°C (102.2°F), and blood pressure 60/40 mm Hg. On physical examination, the patient has delayed capillary refill. Laboratory studies show a pleocytosis and a low glucose level in the patient’s cerebrospinal fluid. Which of the following is the most likely causative organism for this patient’s condition?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app