
Treatment of dimorphic fungal infections — MCQs

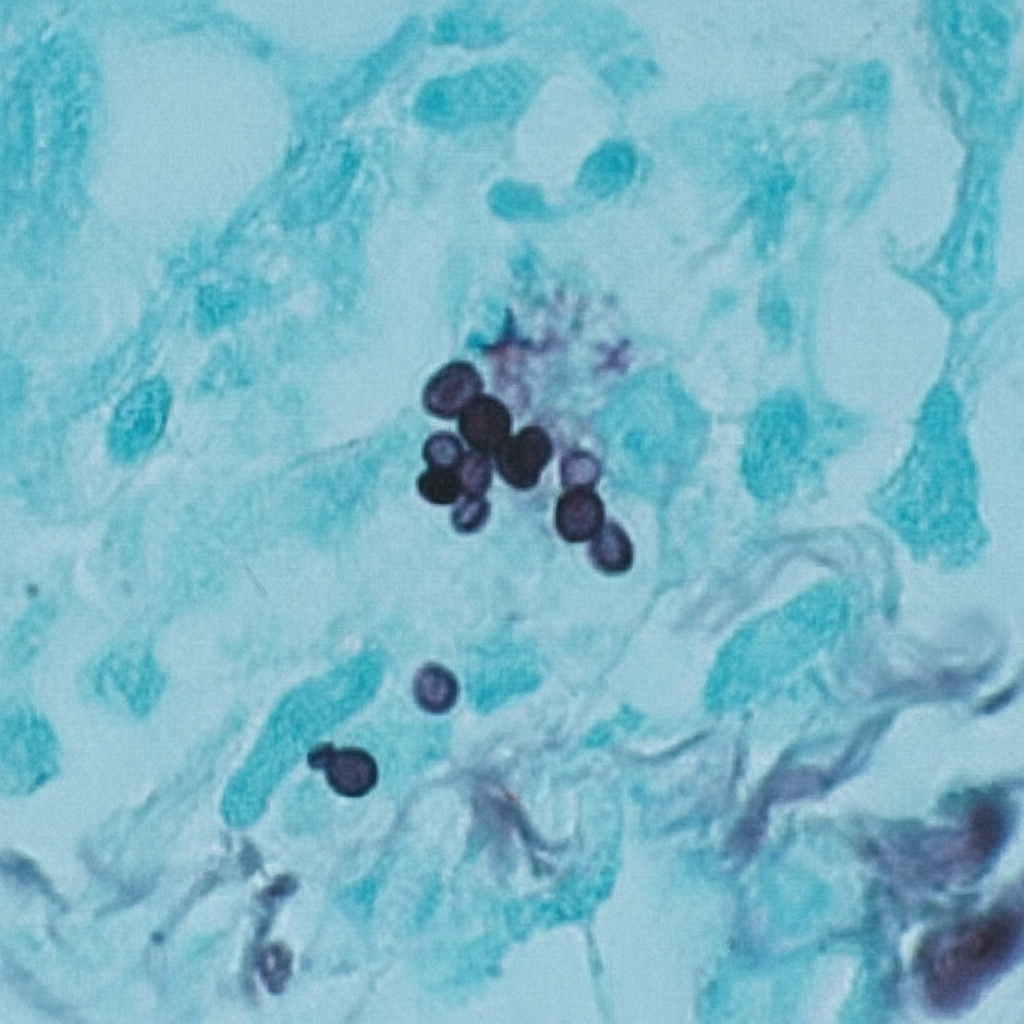
A 44-year-old man comes to the physician because of a 3-week history of productive cough, fever, and lethargy. He also has several skin lesions over his body. His symptoms began 3 weeks after he returned from a camping trip in Kentucky. Three years ago, he underwent kidney transplantation for polycystic kidney disease. Current medications include sirolimus and prednisone. His temperature is 38°C (100.4°F). Diffuse crackles are heard over the lung fields. There are 4 white, verrucous skin patches over his chest and upper limbs. A photomicrograph of a skin biopsy specimen from one of the lesions is shown. Which of the following is the most likely diagnosis?
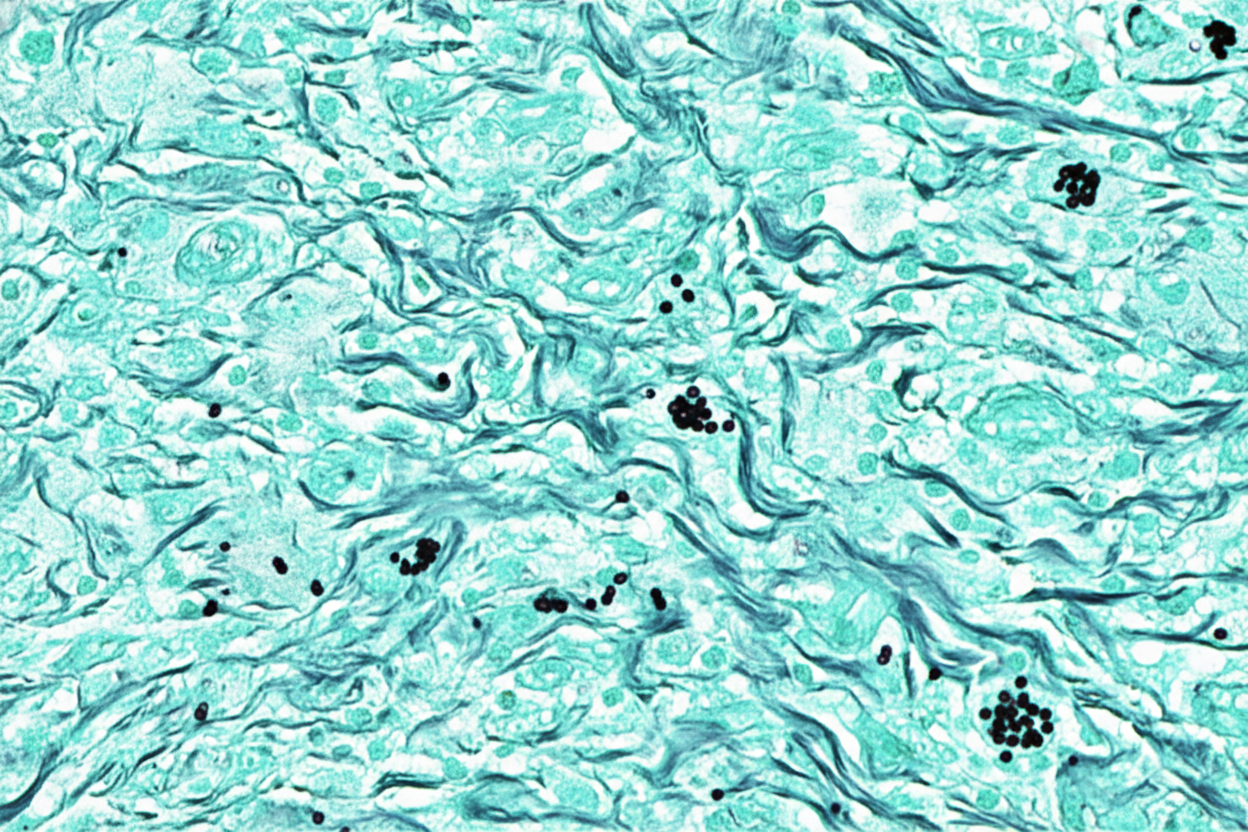
A 52-year-old man comes to the physician because of a 4-day history of a productive cough, shortness of breath, and low-grade fever. He works as a farmer in southern Arizona. Physical examination shows multiple skin lesions with a dark blue center, pale intermediate zone, and red peripheral rim on the upper and lower extremities. There are diffuse crackles on the left side of the chest. An x-ray of the chest shows left basilar consolidation and left hilar lymphadenopathy. A photomicrograph of tissue obtained from a biopsy of the lung is shown. Which of the following is the most likely causal pathogen?
A 25-year-old nulligravid female presents to clinic complaining of abnormal vaginal discharge and vaginal pruritis. The patient's past medical history is unremarkable and she does not take any medications. She is sexually active with 3 male partners and does not use condoms. Pelvic examination is notable for a thick, odorless, white discharge. There is marked erythema and edema of the vulva. Vaginal pH is normal. Microscopic viewing of the discharge shows pseudohyphae and white blood cells. Which of the following is the most appropriate treatment plan?
A 29-year-old woman comes to the military physician because of a 2-day history of fever, joint pain, dry cough, chest pain, and a painful red rash on her lower legs. Two weeks ago, she returned from military training in Southern California. She appears ill. Her temperature is 39°C (102.1°F). Physical examination shows diffuse inspiratory crackles over all lung fields and multiple tender erythematous nodules over the anterior aspect of both legs. A biopsy specimen of this patient's lungs is most likely to show which of the following?
A 73-year-old man presents to the office, complaining of “weird blisters” on his right hand, which appeared 2 weeks ago. The patient says that he initially had a rash, which progressed to blisters. He denies any trauma or known contact with sick people. He is worried because he hasn’t been able to garden since the rash appeared, and he was planning on entering his roses into an annual competition this month. His vital signs are stable. On physical exam, the patient has multiple bullae accompanied by red, papular lesions on his right hand, which progress to his forearm. The right axillary lymph nodes are swollen and tender. What is the treatment for the most likely diagnosis of this patient?
A 74-year-old man is admitted to the medical ward after he developed a fungal infection. He has aplastic anemia. The most recent absolute neutrophil count was 450/µL. An anti-fungal agent is administered that inhibits the fungal enzyme, (1→3)-β-D-glucan synthase, and thereby disrupts the integrity of the fungal cell wall. He responds well to the treatment. Although amphotericin B is more efficacious for his condition, it was not used because of the side effect profile. What was the most likely infection?
A 32-year-old woman presents with three-days of vaginal burning, itching, and pain with intercourse. She is in a monogamous relationship with her husband and has an intrauterine device for contraception. Her past medical history is unremarkable, except for recently being treated with antibiotics for sinusitis. Pelvic exam is remarkable for vulvar excoriations, vaginal wall edema, and thick, white discharge in the vault. Wet mount with KOH staining reveals budding filaments with pseudohyphae and hyphae. Which of the following is the most appropriate treatment?
A 40-year-old farmer from Ohio seeks evaluation at a clinic with complaints of a chronic cough, fevers, and anorexia of several months duration. On examination, he has generalized lymphadenopathy with hepatosplenomegaly. A chest radiograph reveals local infiltrates and patchy opacities involving all lung fields. Fine needle aspiration of an enlarged lymph node shows the presence of intracellular yeast. A fungal culture shows the presence of smooth, thin-walled microconidia and tuberculate macroconidia. Which of the following is the most likely diagnosis?
A 62-year-old man is brought to the emergency department from a senior-care facility after he was found with a decreased level of consciousness and fever. His personal history is relevant for colorectal cancer that was managed with surgical excision of the tumor. Upon admission, he is found to have a blood pressure of 130/80 mm Hg, a pulse of 102/min, a respiratory rate of 20/min, and a body temperature 38.8°C (101.8°F). There is no rash on physical examination; he is found to have neck rigidity, confusion, and photophobia. There are no focal neurological deficits. A head CT is normal without mass or hydrocephalus. A lumbar puncture was performed and cerebrospinal fluid (CSF) is sent to analysis while ceftriaxone and vancomycin are started. Which of the following additional antimicrobials should be added in the management of this patient?
A 30-year-old man is admitted to the hospital with a presumed pneumonia and started on antibiotics. Two days later, the patient shows no improvement. Blood cultures reveal yeast with pseudophyphae. Which of the following cell types is most likely deficient or dysfunctional in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app