
Dimorphic fungi — MCQs

On this page
A 40-year-old farmer from Ohio seeks evaluation at a clinic with complaints of a chronic cough, fevers, and anorexia of several months duration. On examination, he has generalized lymphadenopathy with hepatosplenomegaly. A chest radiograph reveals local infiltrates and patchy opacities involving all lung fields. Fine needle aspiration of an enlarged lymph node shows the presence of intracellular yeast. A fungal culture shows the presence of smooth, thin-walled microconidia and tuberculate macroconidia. Which of the following is the most likely diagnosis?
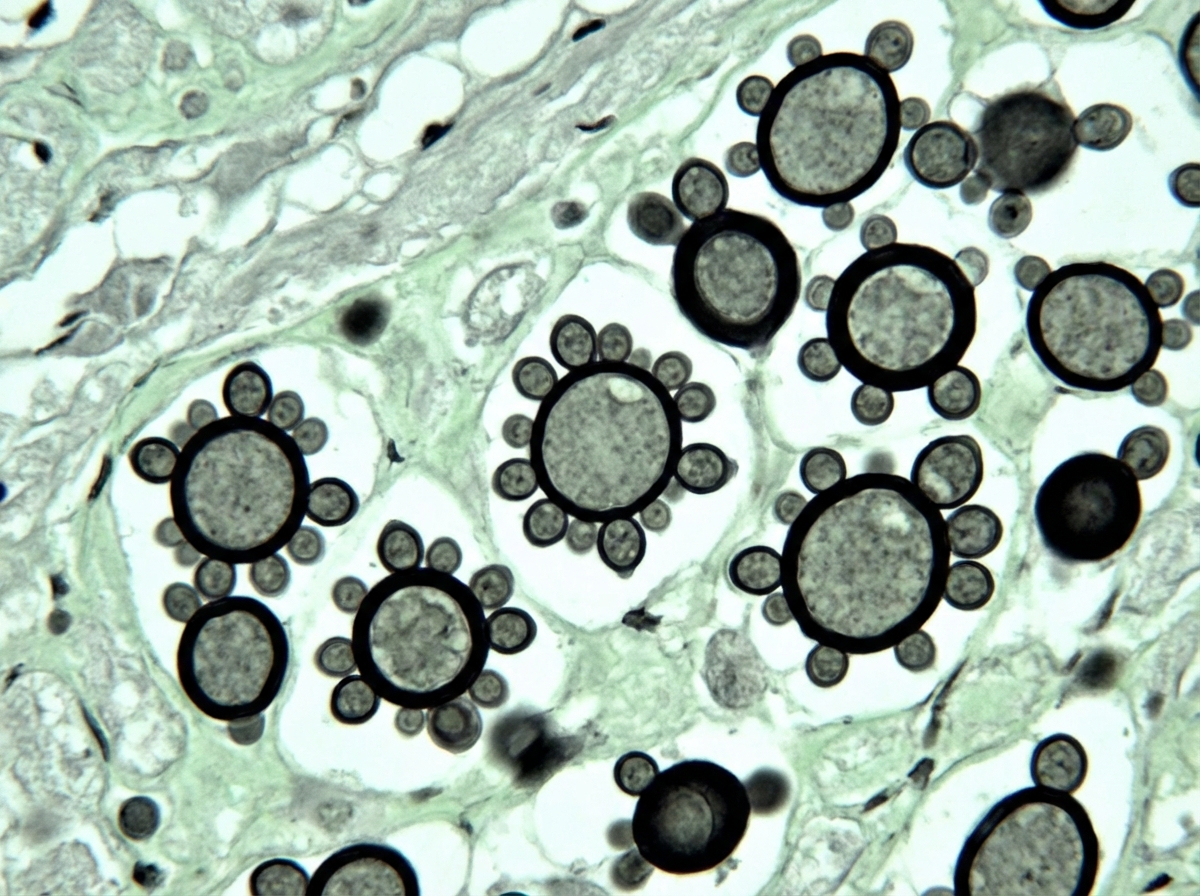
A 32-year-old man comes to the physician because of a 1-week history of fever, weakness, diffuse abdominal pain, and multiple lumps on his body. He has recently returned to the USA from a 3-month agricultural internship in South America. Physical examination shows enlarged superficial cervical and inguinal lymph nodes. There is tender hepatomegaly. A photomicrograph of a liver biopsy sample after methenamine silver staining is shown. Which of the following is the most likely diagnosis?
A 58-year-old woman visits a physician because of fever, chills, dry cough, and a few enlarging masses on her cheeks and neck. Wart-like lesions are present on the nose as shown in the photograph. She reports that she visited the Mississippi area a few months before on a business trip. Her temperature is 38.1°C (100.6°F), the pulse is 80/min, and the blood pressure is 121/78 mm Hg. A fine needle aspirate of the lymph node is sent for pathological investigation. Culture growth shows white colonies on Sabouraud glucose agar (SGA). Which of the following is the most likely causal organism?

A young woman from the Ohio River Valley in the United States currently on corticosteroid therapy for ulcerative colitis presented to a clinic complaining of fever, sweat, headache, nonproductive cough, malaise, and general weakness. A chest radiograph revealed patchy pneumonia in the lower lung fields, together with enlarged mediastinal and hilar lymph nodes. Skin changes suggestive of erythema nodosum (i.e. an acute erythematous eruption) were noted. Because the patient was from a region endemic for fungal infections associated with her symptoms and the patient was in close contact with a person presenting similar symptoms, the attending physician suspected that systemic fungal infection might be responsible for this woman’s illness. Which of the following laboratory tests can the physician use to ensure early detection of the disease, and also effectively monitor the treatment response?
An investigator is studying growth patterns of various fungal pathogens. Incubation of an isolated fungus at 25°C shows branching hyphae with rosettes of conidia under light microscopy. After incubation at 37°C, microscopic examination of the same organism instead shows smooth, white colonies with rounded, elongated cells. Infection with the investigated pathogen is most likely to cause which of the following conditions?
A 50-year-old man from India visits his physician complaining of worsening respiratory symptoms. He states that he was diagnosed with emphysema 4 years ago and that, over the past several months, he has developed a chronic productive cough, dyspnea, fatigue, unexplained weight loss, and night sweats. He notes that he also has other complaints aside from his lung problems, including sharp, intermittent chest pain and joint pain in his elbows and knees. There is also an erythematous rash on both the lower extremities that features raised lesions; it is determined to be erythema nodosum. Cardiac examination reveals a friction rub, and a computed tomography (CT) scan of the chest reveals cavitation of both lung apices. The patient is isolated for the suspicion of active tuberculosis (TB) infection. A purified protein derivative (PPD) test is negative. Sputum sample staining fails to reveal acid-fast bacilli, but it does reveal yeast forms that are replicating by narrow-based budding. Which of the following would aid in making a correct diagnosis in this patient?
A 16-year-old boy presents to his pediatrician because he has noticed white plaques forming on his tongue over the last 5 days. He recently returned from a boy scout trip where he traveled across the country and hiked through the woods. His past medical history is significant for asthma for which he uses an inhaler as needed. He says that during the trip he felt short of breath several times and had to use the inhaler. He also says that several of his friends appeared to get sick on the same trip and were coughing a lot. He has not experienced any other symptoms since returning from the trip. On presentation, he is found to have white plaques on the tongue that can be scraped off. Which of the following is a characteristic of the most likely cause of this patient's disease?
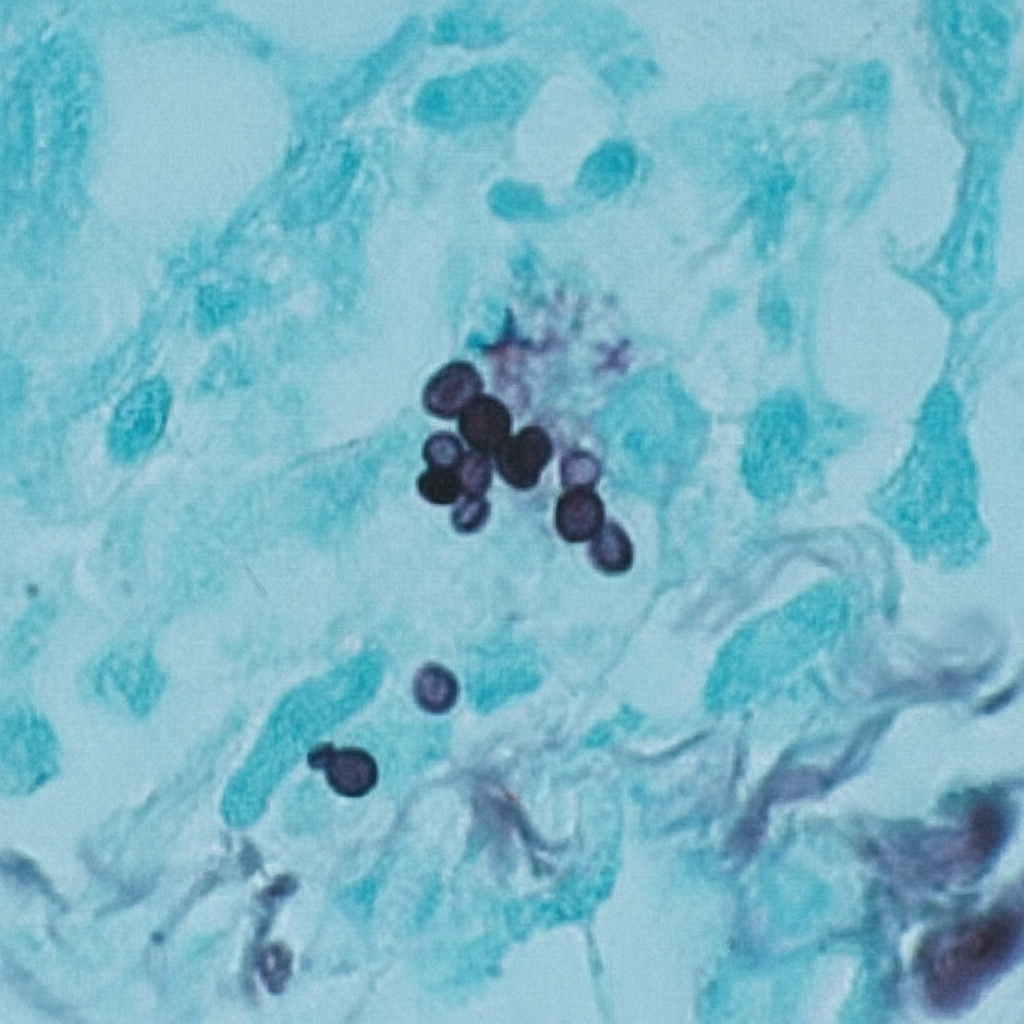
A 44-year-old man comes to the physician because of a 3-week history of productive cough, fever, and lethargy. He also has several skin lesions over his body. His symptoms began 3 weeks after he returned from a camping trip in Kentucky. Three years ago, he underwent kidney transplantation for polycystic kidney disease. Current medications include sirolimus and prednisone. His temperature is 38°C (100.4°F). Diffuse crackles are heard over the lung fields. There are 4 white, verrucous skin patches over his chest and upper limbs. A photomicrograph of a skin biopsy specimen from one of the lesions is shown. Which of the following is the most likely diagnosis?
A 46-year-old woman comes to the physician for a 6-month history of worsening bronchial asthma control. Before this issue began, she only used her salbutamol inhaler once a day. Now, she has to use it multiple times daily and also reports frequent nighttime awakening. Seven months ago, she moved to an apartment that is damp and has mold on some of the walls. The physician injects 0.1 mL of Candida albicans extract on the mid-volar surface of the right arm intradermally. After 48 hours there is a palpable induration of 17 mm. This reaction is most likely a result of release of which of the following substances?
Practice by Chapter
Blastomyces dermatitidis
Practice Questions
Coccidioides immitis/posadasii
Practice Questions
Paracoccidioides brasiliensis
Practice Questions
Sporothrix schenckii complex
Practice Questions
Talaromyces (Penicillium) marneffei
Practice Questions
Dimorphic fungi characteristics
Practice Questions
Geographic distribution of dimorphic fungi
Practice Questions
Clinical presentations of dimorphic fungal infections
Practice Questions
Diagnostic approaches for dimorphic fungi
Practice Questions
Treatment of dimorphic fungal infections
Practice Questions
Host factors in dimorphic fungal infections
Practice Questions
Environmental sources and prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app