
Clinical presentations of dimorphic fungal infections — MCQs

A 44-year-old man comes to the physician because of a 3-week history of productive cough, fever, and lethargy. He also has several skin lesions over his body. His symptoms began 3 weeks after he returned from a camping trip in Kentucky. Three years ago, he underwent kidney transplantation for polycystic kidney disease. Current medications include sirolimus and prednisone. His temperature is 38°C (100.4°F). Diffuse crackles are heard over the lung fields. There are 4 white, verrucous skin patches over his chest and upper limbs. A photomicrograph of a skin biopsy specimen from one of the lesions is shown. Which of the following is the most likely diagnosis?
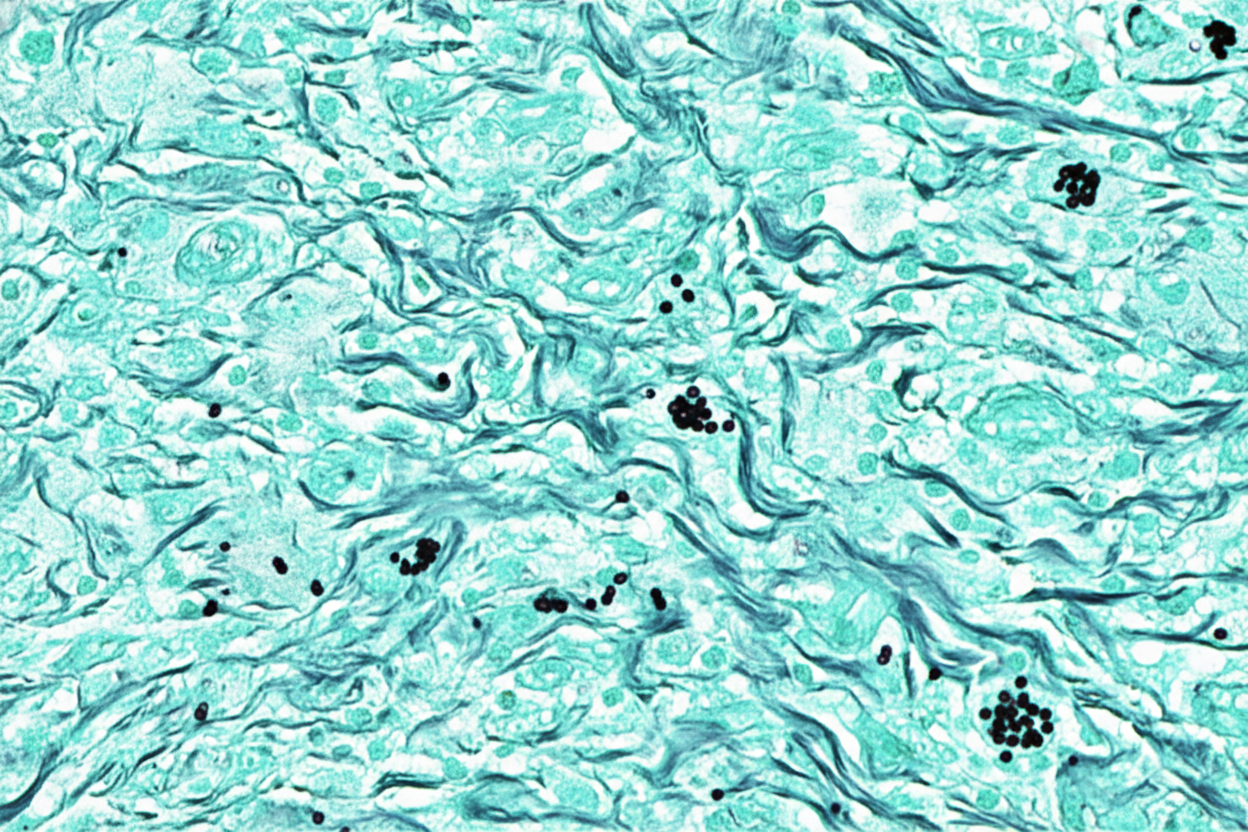
A 52-year-old man comes to the physician because of a 4-day history of a productive cough, shortness of breath, and low-grade fever. He works as a farmer in southern Arizona. Physical examination shows multiple skin lesions with a dark blue center, pale intermediate zone, and red peripheral rim on the upper and lower extremities. There are diffuse crackles on the left side of the chest. An x-ray of the chest shows left basilar consolidation and left hilar lymphadenopathy. A photomicrograph of tissue obtained from a biopsy of the lung is shown. Which of the following is the most likely causal pathogen?
An investigator is studying growth patterns of various fungal pathogens. Incubation of an isolated fungus at 25°C shows branching hyphae with rosettes of conidia under light microscopy. After incubation at 37°C, microscopic examination of the same organism instead shows smooth, white colonies with rounded, elongated cells. Infection with the investigated pathogen is most likely to cause which of the following conditions?
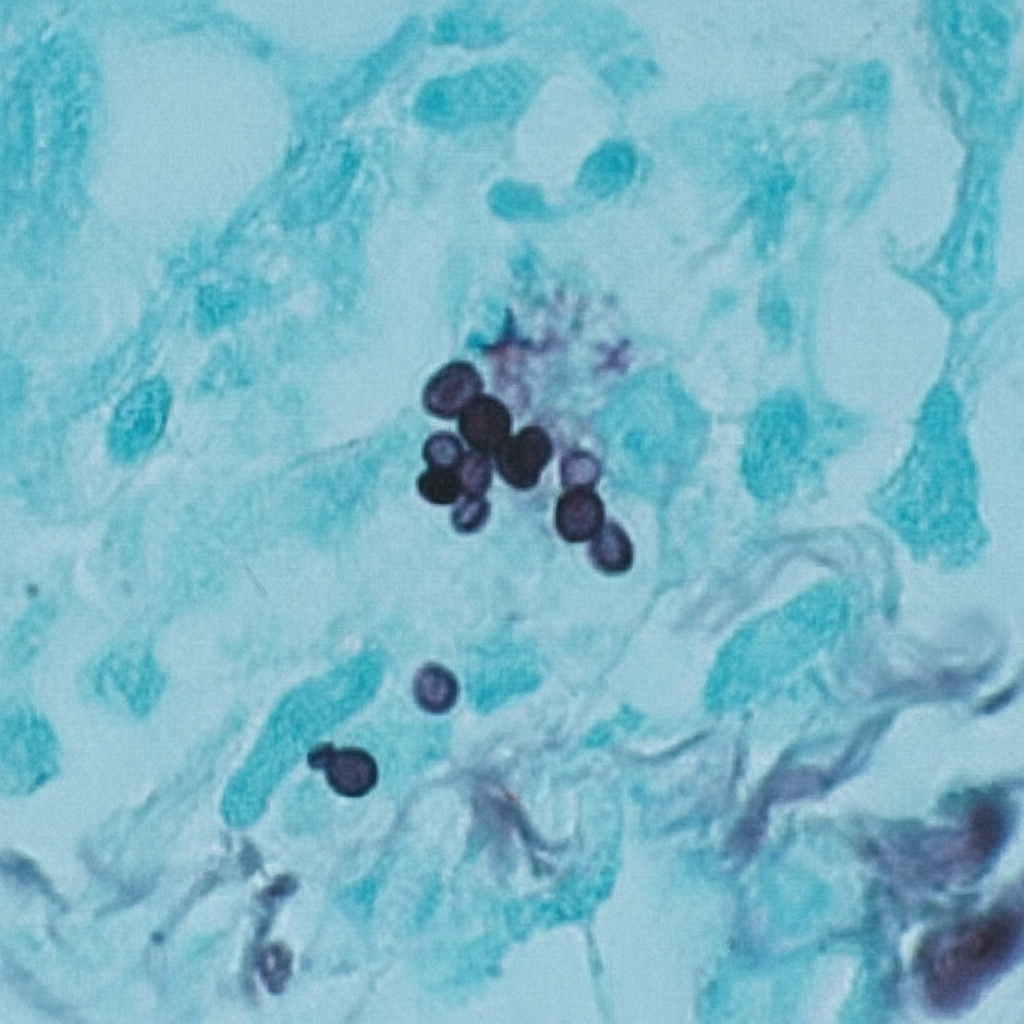
A 47-year-old woman comes to the physician because of a 3-day history of fever, fatigue, loss of appetite, cough, and chest pain. Physical examination shows diffuse inspiratory crackles over the left lung field. An x-ray of the chest shows hilar lymphadenopathy and well-defined nodules with central calcifications. Urine studies show the presence of a polysaccharide antigen. A biopsy specimen of the lung shows cells with basophilic, crescent-shaped nuclei and pericellular halos located within macrophages. This patient's history is most likely to show which of the following?
A 43-year-old type 1 diabetic woman who is poorly compliant with her diabetes medications presented to the emergency department with hemorrhage from her nose. On exam, you observe the findings shown in figure A. What is the most likely explanation for these findings?

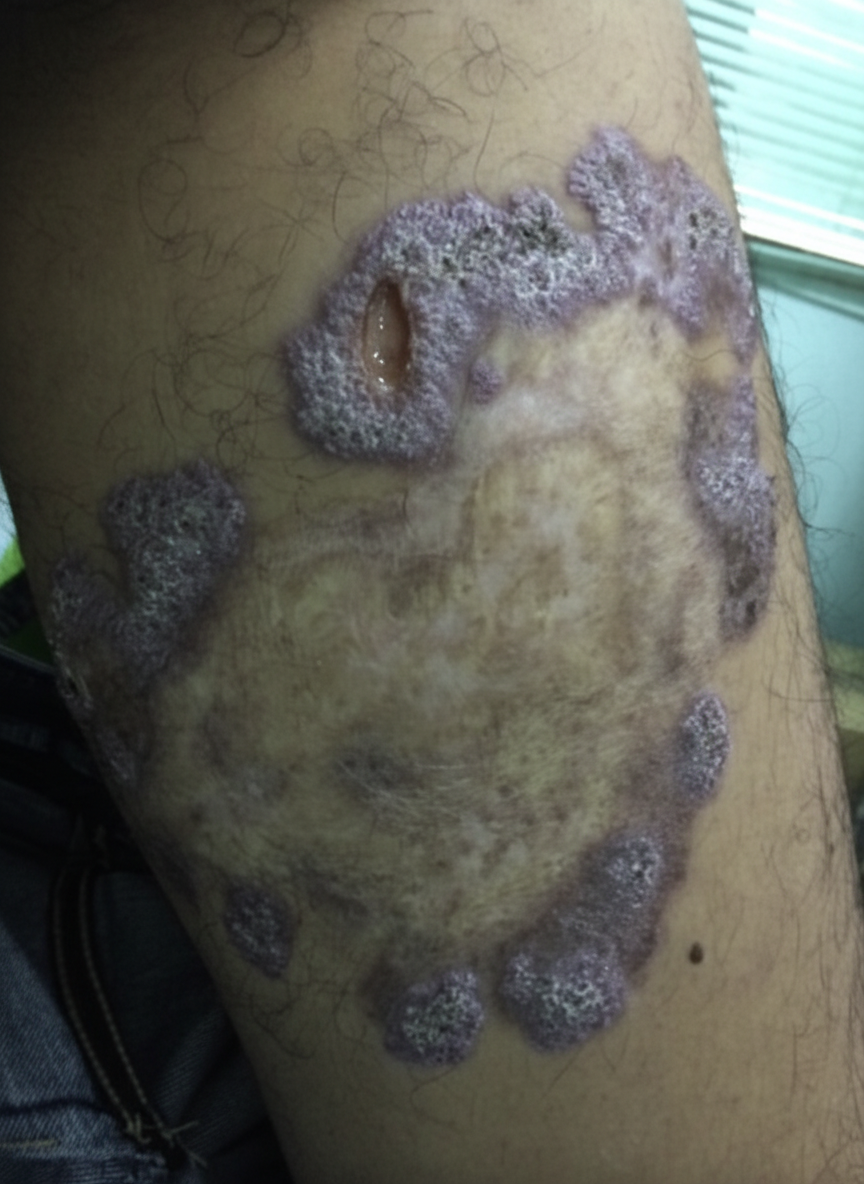
A 54-year-old gardener with diabetes mellitus from the Northeast Jilin Province in China acquired a small scratch from a thorn while working in his flower garden. After 3 weeks, he noticed a small pink, painless bump at the site of a scratch. He was not concerned by the bump; however, additional linearly-distributed bumps that resembled boils began to appear 1 week later that were quite painful. When the changes took on the appearance of open sores that drained clear fluid without any evidence of healing (as shown on the image), he finally visited his physician. The physician referred to the gardener for a skin biopsy to confirm his working diagnosis and to start treatment as soon as possible. Which of the following is the most likely diagnosis for this patient?
A 40-year-old farmer from Ohio seeks evaluation at a clinic with complaints of a chronic cough, fevers, and anorexia of several months duration. On examination, he has generalized lymphadenopathy with hepatosplenomegaly. A chest radiograph reveals local infiltrates and patchy opacities involving all lung fields. Fine needle aspiration of an enlarged lymph node shows the presence of intracellular yeast. A fungal culture shows the presence of smooth, thin-walled microconidia and tuberculate macroconidia. Which of the following is the most likely diagnosis?
A 58-year-old man presents with a high-grade fever, throbbing left-sided headache, vision loss, and left orbital pain. He says that his symptoms started acutely 2 days ago with painful left-sided mid-facial swelling and a rash, which progressively worsened. Today, he woke up with complete vision loss in his left eye. His past medical history is significant for type 2 diabetes mellitus, diagnosed 5 years ago. He was started on an oral hypoglycemic agent which he discontinued after a year. His temperature is 38.9°C (102.0°F), blood pressure is 120/80 mm Hg, pulse is 120/min, and respiratory rate is 20/min. On examination, there is purulent discharge from the left eye and swelling of the left half of his face including the orbit. Oral examination reveals extensive necrosis of the palate with a black necrotic eschar and purulent discharge. Ophthalmic examination is significant for left-sided ptosis, proptosis, and an absence of the pupillary light reflex. Laboratory findings are significant for a blood glucose level of 388 mg/dL and a white blood cell count of 19,000 cells/mm³. Urinary ketone bodies are positive. Fungal elements are found on a KOH mount of the discharge. Which of the following statements best describes the organism responsible for this patient’s condition?
A 29-year-old woman comes to the military physician because of a 2-day history of fever, joint pain, dry cough, chest pain, and a painful red rash on her lower legs. Two weeks ago, she returned from military training in Southern California. She appears ill. Her temperature is 39°C (102.1°F). Physical examination shows diffuse inspiratory crackles over all lung fields and multiple tender erythematous nodules over the anterior aspect of both legs. A biopsy specimen of this patient's lungs is most likely to show which of the following?
A 3-month-old girl is brought to the emergency department because of a 2-day history of progressive difficulty breathing and a dry cough. Five weeks ago, she was diagnosed with diffuse hemangiomas involving the intrathoracic cavity and started treatment with prednisolone. She appears uncomfortable and in moderate respiratory distress. Her temperature is 38°C (100.4°F), pulse is 150/min, respirations are 50/min, and blood pressure is 88/50 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 87%. Oral examination shows a white plaque covering the tongue that bleeds when scraped. Chest examination shows subcostal and intercostal retractions. Scattered fine crackles and rhonchi are heard throughout both lung fields. Laboratory studies show a leukocyte count of 21,000/mm3 and an increased serum beta-D-glucan concentration. An x-ray of the chest shows symmetrical, diffuse interstitial infiltrates. Which of the following is most likely to confirm the diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app